Summary of the findings
Image: Asaf Klinger / Imagebank.sweden.se
This report synthesises evidence from three complementary data sources:
- a structured literature review of meta‑analyses and systematic reviews published since 2010,
- an intervention mapping of psychosocial programmes evaluated in Nordic and international evidence portals, and
- insights from Nordic expert discussions conducted in 2025–2026.
All results were organised according to the WHO maternal well-being framework, which conceptualises perinatal psychosocial well-being across six interlinked domains. The framework's domains provided a broad and multidomainal organising structure, making visible a wider range of risk and protective factors than narrower clinical definitions would allow.
The findings are consistent with existing literature in showing that perinatal psychosocial well-being is shaped by an accumulation of interacting factors spanning health, relationships, safety, autonomy, culture and the quality of care, and that these factors rarely operate in isolation. Families facing the greatest vulnerabilities tend to encounter multiple risk factors simultaneously, while adequate support may mitigate them.
Scope of the evidence base
Most of the reviewed literature primarily targeted mothers’ perspectives. While some literature also addressed the experiences of both parents, and some exclusively focused on fathers, the mother’s viewpoint remained a central focus in many of the articles. Although the research literature uses terminology that primarily refers to mothers and fathers or to women and men, families and parenthood in society also include other constellations. This broader understanding should be considered when interpreting the results of this review.
Altogether, 33% of the reviewed articles primarily focused on parents' mental health and investigated themes related to mental health issues, such as depression, PTSD and perinatal psychological disorders, as well as social challenges, such as the mental health issues of migrants. Furthermore, 54% of the articles addressed mental health either as an outcome variable or as a mediating/moderating factor, indicating that the topic has been addressed in international research. Although no separate literature searches were conducted specifically on interventions, some effectiveness studies still emerged through the literature search carried out.
Research from the child’s perspective remains limited, despite the frequent emphasis on child well-being as a central objective. Although the aim is equally to ensure the child’s needs, health and safe development, services and interventions mostly concentrate on mothers or parents.
In this report, only meta-analyses and systematic reviews were included, which limited the number of Nordic studies. Altogether, 35% of the investigated articles included studies from the Nordic region, and the results aligned with other high-income countries included.
Limitations of the report
This review has several limitations. Firstly, it relies on a broad but necessarily selective evidence base compiled within a short time frame, which may result in some analyses being underdeveloped. Several important topics, such as prematurity, low birth weight, feeding difficulties, adolescent pregnancies and the impact of the pandemic, were excluded due to the scope and the required specialised expertise. Focusing on English-language systematic reviews and meta-analyses limited the inclusion of Nordic evidence, which may reduce regional applicability. The search strategy only partially captured literature on early interaction, attachment and bonding, and despite supplementation later in the process, the evidence remains fragmented. The review is also constrained by its parent-centred perspective, the lack of experiential input from families and the exclusion of broader environmental and developmental factors affecting infants. Finally, the assessment of psychosocial interventions is limited by variability across evaluation systems, the narrow set of portals searched and the fact that information on which interventions are currently implemented in Nordic contexts is incomplete. A more detailed list of limitations is provided; please see Appendix 6.
Identified evidence gaps
The identified research focused on depression, leaving other conditions less understood. Many under-researched populations merit attention. The mental health of fathers and partners is interlinked with that of mothers, but is often studied far less, and cultural/ethnic minorities or refugee families who face unique stressors and are underrepresented in research samples were noted as gaps. There is a significant evidence gap regarding knowledge related to the psychosocial well-being of Sámi people during the perinatal period. Cumulative risk factors and the role of social inequalities should be more broadly investigated. Table 13 summarises the identified gaps in evidence.
Methodologically, there is a call for the use of standardised measures (for issues such as pregnancy anxiety or bonding disorders) and the inclusion of diverse data sources. Longitudinal and robust designs are needed to investigate long-term outcomes for children and their families.
The literature demonstrated limited evidence on: | Additional evidence gaps mentioned in Nordic expert discussions |
|---|---|
|
|
Table 13. Identified evidence gaps.
Key risk and protective factors during the perinatal period
The findings of this report suggest that the six interconnected domains provided by the WHO maternal well-being framework (Le Lez et al., 2025) of health and nutrition, relationships and connectedness, security, safety and a sustainable environment, autonomy, agency and resilience in parenting, culture and values, and the provision and experience of care together shape the well-being of parents and children.
For instance, parental mental health issues, social difficulties such as loneliness, and financial strain may impact both parent–child interactions and the wider family environment. Addressing these issues usually necessitates a coordinated, multi-level approach across services and support systems.
The findings also highlight areas where support structures could be improved, such as meeting the needs of culturally and linguistically diverse families, engaging fathers, responding to trauma and family violence and addressing broader structural inequalities. Eight central risk factors were identified across the literature, which are described in the following section. These summaries are based on the evidence presented in the preceding sections.
These factors have been highlighted in the literature, and interventions aimed at enhancing them should play an important role in strategies that seek to create optimal conditions for psychosocial well-being during the perinatal period.
Mental health
The review of the literature revealed that parental mental health problems are key risk factors for the well-being of both parents and children. Perinatal depression and anxiety disorders are the most common perinatal mental health disorders and have strong comorbidity. They are associated with a higher risk of adverse outcomes for children, including preterm birth, low birth weight, regulatory and sleep problems and interaction disorders, as well as and later developmental, behavioural and mental health problems. In addition to these, the literature review identified several other disorders, such as PTSD, obsessive–compulsive disorder, panic disorder, eating disorders and serious mental health illnesses, that are clearly linked to perinatal well-being but are less commonly identified in healthcare settings than depression.
Perinatal mental health challenges rarely arise from a single cause; rather, they reflect a complex interplay of individual, relational and structural factors that often overlap and reinforce one another. Risk factors often accumulate, and a history of mental health disorders, ACE experiences, intimate partner violence, socioeconomic stress, perinatal losses and somatic morbidity significantly increase the risk of depression, anxiety and trauma symptoms. These interconnected factors influence not only parental mental health but also early attachment, child development and family stability.
Fathers also experience perinatal mental health symptoms, yet their well-being is rarely monitored. Some support and interventions are offered to both parents, but most of them only mention mothers as the target group.
Protective factors for mental health include the support of a good partnership and a close circle of friends and family. Moreover, individuals’ internal resources, such as resilience, optimism and reflective capacity, protect against depression and anxiety while supporting secure attachment and family stability. In addition, financial and housing security, adequate sleep, physical health and low-threshold psychological support may promote resilience and safeguard mental health for both parents and children. Adequate early identification, evidence-based treatment, a sensitive and trauma-informed therapeutic relationship, as well as support received by fathers and their good mental health were identified as factors that can support the well-being of the whole family.
Perinatal trauma and loss
Loss and traumatic experiences, such as complications in pregnancy and negative childbirth experiences, perinatal loss and previous traumatic events, significantly increase the risk of depression, anxiety and PTSD in parents. Negative experiences or a perceived lack of control during childbirth are associated with poorer mental well-being.
Protective factors that can reduce the risk of psychological symptoms included social support, compassionate encounters with healthcare personnel and the opportunity to participate in decision-making during childbirth and care.
Transition to parenthood and the experience of competence
The literature review revealed that transitioning to parenthood is a psychologically stressful transition phase in which expectations, norms and the personal life history have a strong impact on the experience of competence. For mothers, studies have described how unrealistic parenting expectations, body image pressures, breastfeeding pressures and social comparison increase anxiety, depressive symptoms and feelings of inadequacy. Fathers, on the other hand, repeatedly describe feelings of exclusion, a lack of information and insufficient consideration of their experiences, which weakens their sense of competence and increases stress. The well-being and perceived competence of both parents are linked to the early development of the child and parent–child interaction.
Protective factors include the experience of being heard, being able to participate in decision-making regarding pregnancy, childbirth and early care, and receiving understandable information and support. Psychological resilience, effective coping strategies, positive self-esteem and realistic expectations of parenthood are associated with better adaptation. Interventions that support resilience, stress management, peer support and comprehensive support for living conditions (finances, housing) appear to be protective factors, especially in socioeconomically vulnerable groups.
Social relationships and support
The review of the literature demonstrated that social relationships and informal support networks are among the strongest protective factors during the perinatal period. Emotional and practical support from a partner, high‑quality couple functioning and cooperative co‑parenting reduce the risk of depression, anxiety and stress in both mothers and fathers. Conversely, relationship conflict, single parenthood and loneliness are consistently linked with poorer mental‑health outcomes. Loneliness is a particularly salient risk factor and is associated with increased psychological distress, lower parenting confidence and reduced help‑seeking.
Protective factors include natural communities, an extended family and supportive close relationships, which can buffer stress, reduce isolation and strengthen parents’ everyday coping. Group‑based interventions and peer‑support elements enhance social connectedness and reduce stigma, and they should be promoted in both universal and targeted formats.
Parent–infant relationship
The review of the literature revealed that early parent–infant interaction, bonding and the development of secure attachment are central to the child’s emotional, social and self‑regulation development. Parental mental health difficulties and illnesses, fatigue, trauma symptoms, neurodevelopmental conditions and substance‑use problems are associated with reduced sensitivity to infant cues and more fragmented interaction. Specific circumstances such as prematurity, neonatal intensive care admission, perinatal loss or birth‑related PTSD may delay bonding and increase vulnerability in the early relationship.
Risk factors often overlap, and parental depression or anxiety, previous trauma, chronic stress and a lack of social support can further weaken the quality of early interaction. These factors increase the likelihood of difficulties in regulation, feeding, sleep and early developmental trajectories.
Protective factors include sensitive, consistent and responsive caregiving, which can act as strong buffers, even when parents experience psychological symptoms. Interventions focusing on parent–child interaction (for example, video-based and home‑visiting models) strengthen parental sensitivity and mentalisation, reduce interactional stress and support secure attachment. Positive shared moments, skin‑to‑skin care and structured observation of infant behaviour further reinforce bonding and resilience in both the parent and child.
Migrant and minority families
Migrant and minority families often face cumulative stressors during the perinatal period. Language barriers, discrimination and pre‑migration trauma, among other risks, increase the risk of perinatal depression, anxiety and trauma‑related symptoms. Sexual and gender minority parents may experience stigma, limited service accessibility and non‑inclusive care, which further heighten vulnerability.
Protective factors highlight culturally sensitive and respectful care, access to multilingual information, the availability of interpreting services and opportunities to maintain cultural identity and community ties. Protective factors also include strong family and community networks, maintaining one's own traditions, peer support and spiritual communities, which can significantly support well-being and coping during the perinatal period. Alongside these, culturally sensitive service guidance is important so that parents can make use of both their own cultural resources and professional support. Inclusive service practices, culturally adapted materials and collaboration with community organisations help strengthen parental well-being. However, the intervention mapping revealed a clear gap: no culturally adapted perinatal mental health intervention programmes with demonstrated effectiveness were identified in the Nordic countries, despite the known benefits of culturally sensitive approaches.
Social inequalities and cumulative risks
The literature review demonstrated that many families experience interconnected and mutually reinforcing risk factors. Adverse childhood experiences, poverty, unemployment, housing instability and neighbourhood disadvantage are social disadvantages that may be linked with parental mental health or substance‑use problems and cumulate adversity. They increase the likelihood of perinatal distress and adverse outcomes for children. Children in families with a cumulative risk are more likely to experience regulatory, developmental and behavioural difficulties. Parents with such histories may also have less informal support and a reduced help‑seeking ability. Intimate partner violence during pregnancy or the postpartum period is a significant risk factor for family well-being, safety and child development. It undermines the parent's sense of security and increases the likelihood of depression and trauma symptoms. A safe, non-violent home environment is therefore a key protective factor for the well-being of both parents and children, and this is why the early identification of at-risk families and the provision of support are particularly important.
Protective factors include positive early experiences, safe and supportive relationships, stable living conditions, reliable social protection and opportunities to address trauma within a trustworthy care relationship. These can mitigate the effects of cumulative risk. Effective programmes identified in intervention mapping combine parental support, child‑centred interventions and practical assistance to strengthen family stability and long‑term resilience.
Role of the service system
The service system can either protect or exacerbate risks. Fragmented pathways, inconsistent screening and culturally insensitive practices delay identification, whereas trauma‑informed, coordinated and accessible services support early detection and engagement.
Conversely, universal and accessible services, regular home‑visiting, continuity of care and high‑quality therapeutic relationships are protective. Trauma‑informed and culturally sensitive care, clear care pathways and coordinated multi‑professional collaboration improve early identification and strengthen parental trust in services.
Protective factors include early detection and evidence-based treatment for risks, high‑quality therapeutic alliances and integrated service structures. These can provide important foundations for safe, equitable and timely support. This report, combining reviews of the literature, intervention portals and Nordic expert discussions, demonstrates that while the improvement of professional competence is often supported, stepped-care models (see Figure 4) and specialised units remain unevenly available in the Nordic countries.
Key protective factors at different support levels are presented in Figure 3.
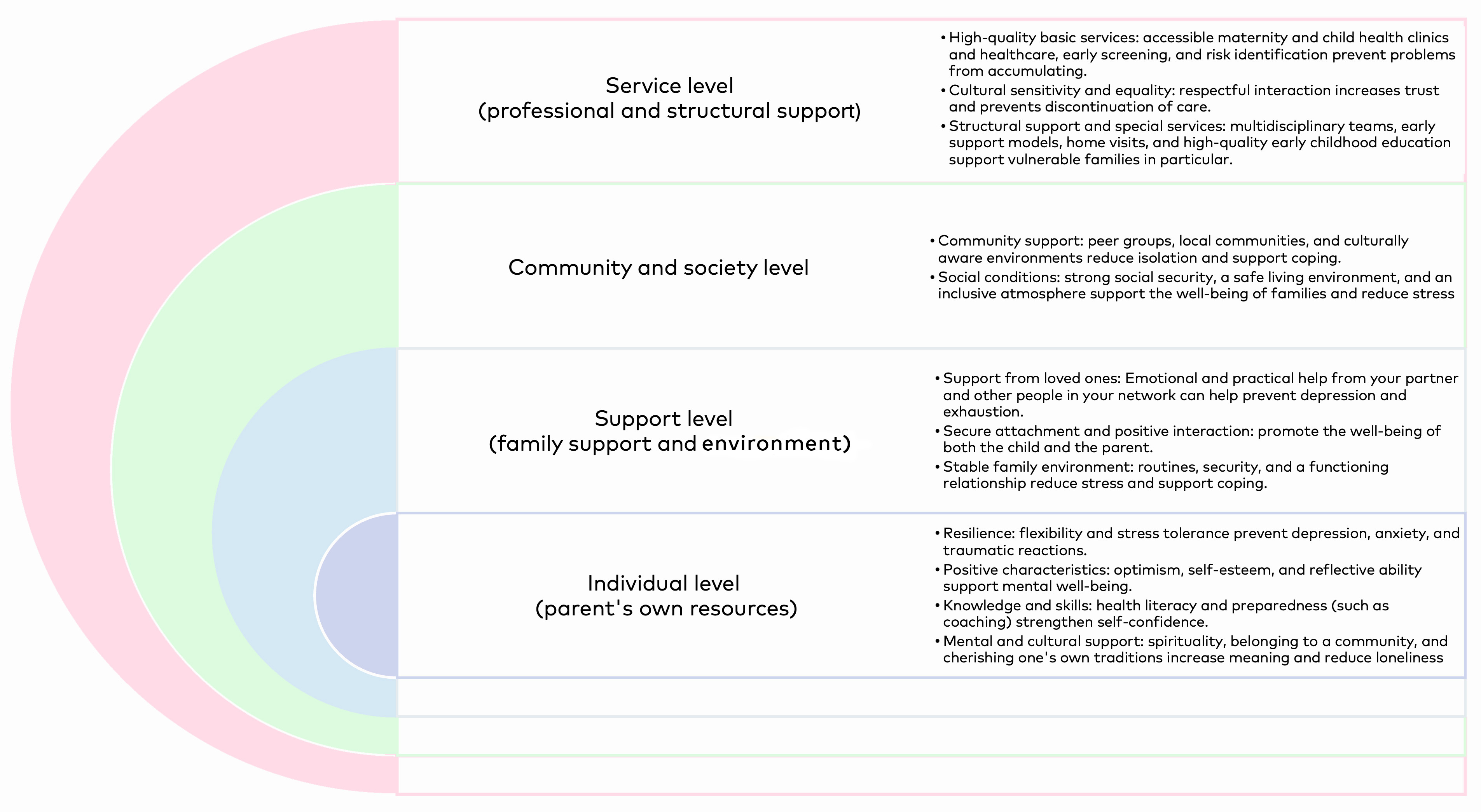
Figure 3. Identified protective factors at different levels.
Key findings from psychosocial intervention mapping
The aim of the psychosocial intervention mapping is to examine how well the interventions with graded effectiveness meet the identified risk factors and needs for psychosocial support and where the biggest gaps lie. Although this report focuses on psychosocial interventions with research evidence that has been evaluated in the open-source intervention information portals, it should be noted that this review does not provide a complete picture of the care and support available. For example, specialised care meets some of the identified risks and the care is beyond psychosocial support offered in intervention programmes (for example, psychotic disorders or child developmental challenges are treated in specialised care).
A total of 28 structured interventions with evaluated effectiveness in Nordic context were identified in the intervention information portal mapping. They included universal (8 interventions), risk group-targeted (13 interventions) and therapeutic (7) interventions. In the analysis phase, we categorized the interventions covering the perinatal period into WHO‑based domains, which proved challenging and at times somewhat artificial due to the complexity of the phenomena and their overlapping nature. Table 14 presents all the interventions identified in the Nordic intervention portals reviewed (not additional international portal findings included).
Table 14. Identified psychosocial intervention with Nordic effectiveness grading.

The focus of this report is on interventions evaluated in publicly available online intervention information portals, with evidence ranging from promising to strong. If a psychosocial intervention has not yet been sufficiently studied in the Nordic context, it cannot be stated with certainty that the intervention will produce the desired effects. More detailed information on the interventions is available in each domain chapter and the related appendices (3–4).
As the field is broad and evidence continues to develop, interventions not yet included in information portals or lacking well‑established Nordic evidence may be missing from the review. In cases of urgent need, interventions with promising or moderate evidence may still be appropriate, and some needs may be addressed by adapting well‑established interventions from outside the Nordic region.
Expert discussions emphasised that the lack of care pathways and stepped-care models is a major challenge in perinatal mental health services. Although effective interventions exist, implementation often fails without structures that guide timely and targeted support. Stepped care provides a clear framework in which the intensity of support increases according to need, helping ensure efficient resource use and appropriate support at the right time.
Intervention gaps in relation to identified needs
Several gaps were identified between recognised risks and the interventions with an effectiveness evaluation. These gaps refer to needs identified in the literature and expert discussions that did not match any interventions with assessed effectiveness (see inclusion criteria in the chapter Psychosocial intervention information portal mapping). The gap analysis was based on the report’s data sources. When the identified needs did not correspond to any intervention included in the portals or when the available interventions lacked sufficient evidence these were categorised as gaps.
To support clarity, the identified gaps are presented in Table 15 according to the six domains used throughout the report (Health & nutrition; Relationships & connectedness; Security, safety & a sustainable environment; Autonomy & resilience; Culture & values; Provision & experience of care). This domain‑based structure allows the reader to see how the unmet needs cluster within different areas of parental and infant psychosocial well‑being and where the largest discrepancies between needs and evidence‑based interventions occur
More detailed information on the intervention mapping results, including the domain‑organised table and the alignment between risks, existing interventions and identified gaps, can be found in the sections presenting the portal review results and Appendices 3–4.
Effective intervention gaps aligned with identified needs | Additional information |
|---|---|
Health and nutrition (parental): • eating disorders • OCD • parental trauma • PTSD • neuropsychiatric challenges • bipolar disorder • schizophrenia • other psychotic disorders • substance abuse • experiences of perinatal loss • negative or traumatic childhood experiences • child development problems • disabilities and physical limitations • overweight | Some of health-related risks are treated in specialized health care, as for example psychotic disorders, which may explain the absence of psychosocial support programmes. Some of the risks may be overlapping with other domain risks and the support may sometimes meet also these needs. When observing British and American intervention portals, there were effective interventions mentioned also for parental trauma, PTSD, substance abuse, and overweight. |
Relational and connectedness: • lack of social support • challenges in relationship (between couples) • single parents | Some of these risks may be met with the interventions cathegorized under other domains, for example the programmes providing peer-support may also tackle lack of social support even if it is not the primary focus of the intervention. In British and American intervention portals, the interventions with effectiveness support were found also to lack of social support and challenges in couples relationships, which were not in focus in the effective interventions in Nordic context. |
Security, safety and sustainable environment: • experiences of disasters | Interventions measured as effective in British or American portals did not identify experiences of disasters as a primary target either. |
Autonomy, agency and resilience: • disable parents • negative body image | Interventions measured as effective in British or American portals did not identify disable parents or negative body image as primary targets in psychosocial interventions. |
Culture and values: • immigrants, refugees, and asylum seekers • sexual and gender minorities • other cultural minorities | British and American portals had only one intervention (Family Spirit) with effectiveness meeting the risk of cultural minority groups. Other minority groups were not targeted in effective interventions. |
Table 15. The gaps in effective psychosocial interventions identified are described according to six domains.