Introduction
Image: iStock
The aim of this report is to provide an overview of needs and gaps to strengthen psychosocial well-being during the first 1000 days of life. It identifies current needs for psychosocial support and promotes the systematic use of effective, evidence-based interventions for expectant parents, children under two years of age and their families across the Nordic region. The report synthesises literature, intervention reviews and expert insights to inform future implementation strategies in the Nordic countries. This report is part of the ongoing work of the Nordic Network about the child’s first 1000 days – a healthy start in life, which builds upon the earlier The First 1000 Days in the Nordic Countries project 2019–2022.
The First 1000 Days is a concept that refers to the period from conception to first two years of a child’s life, and its importance is well recognised in research, policy and practices. These first years in a child's life are an essential foundation for development and lifelong health and well-being. In the early years, brain development is rapid and exceptionally receptive to influences, and it forms the foundation for cognition, regulative functions and academic achievements (Shonkoff et al., 2012). Robust evidence demonstrates that early experiences affect health and well-being, as well as behaviour and social relationships in later life (Darling et al., 2020).
In this report: The perinatal period refers to the time from pregnancy through childbirth and the postnatal period, extending to the child’s first two years of life. This definition aligns with the First 1000 Days framework and captures the critical developmental and psychosocial transitions that affect parental and child well-being. The psychosocial well-being refers to a multidomainal state that encompasses an individual’s psychological, emotional and social functioning, which includes the capacity to cope with everyday stress, maintain meaningful social relationships, develop personal and cognitive strengths, and function effectively as a member of society (Kumar, 2020).
In this report: The perinatal period refers to the time from pregnancy through childbirth and the postnatal period, extending to the child’s first two years of life. This definition aligns with the First 1000 Days framework and captures the critical developmental and psychosocial transitions that affect parental and child well-being. The psychosocial well-being refers to a multidomainal state that encompasses an individual’s psychological, emotional and social functioning, which includes the capacity to cope with everyday stress, maintain meaningful social relationships, develop personal and cognitive strengths, and function effectively as a member of society (Kumar, 2020).

Background
The Nordic network about the child’s first 1000 days – a healthy start in life
The Nordic network about the child’s first 1000 days - a healthy start in life brings together experts from all Nordic countries and the Nordic Welfare Centre under a mandate from the Nordic Council of Ministers to strengthen knowledge sharing and collaboration that support children’s development and well-being from pregnancy to two years of age (NWC). The network promotes collaboration and knowledge sharing among the Nordic countries on early childhood development, emphasising the need for policies that prioritise the early years, including the period of pregnancy. The network disseminates research, knowledge and understanding about the first 1000 days of life and supports actions that can strengthen Nordic research and address risk factors more effectively through evidence‑based psychosocial interventions. Representatives from Denmark, Finland, Iceland, Norway and Sweden, as well as the Nordic Welfare Centre, are members of the Network. The work of the network contributes to the implementation of Vision 2030 of the Nordic Council of Ministers and the United Nations’ Agenda 2030 for Sustainable Development, which both recognise that good health, including mental health of the child and its family, is essential to the child’s life and development (Nordic Council of Ministers, 2020).
The network was formed in 2023 to follow up on the recommendations that were developed during the project “The First 1000 Days in the Nordic Countries”, which was implemented in 2019–2022 with funding from the Nordic Council of Ministers. This project identified both strengths and challenges in supporting young children's health and well-being in the Nordic countries. Each Nordic country has its own structure and universal healthcare and social services, in which prenatal and infant healthcare services are well established, free of charge and accessible to all families. The guidelines for services in the Nordic countries emphasise supporting the child's health and development, as well as the parent–child relationship, from pregnancy onwards. They also emphasise the systematic identification of risks and an early response to them (Daníelsdóttir & Ingudóttir, 2020, 2022). With their strong welfare systems, the Nordic countries are thus well positioned to ensure optimal conditions for child development.
Despite these strengths, the First 1000 Days in the Nordic Countries project (2019–2022) revealed significant gaps. Few of the reported psychosocial interventions that are in use in the perinatal period have been rigorously evaluated. Thus, the effectiveness of many widely implemented interventions remains unknown. Existing evidence-based interventions do not cover all relevant problem areas, and interventions with strong evidence are not consistently disseminated. The lack of comprehensive training structures and implementation plans further limits the adoption of validated approaches in practice (Martinussen & Kurki, 2021).
To address these challenges, there is a clear need for Nordic collaboration to encourage the implementation of psychosocial support across all levels of care. Joint efforts can pool resources, align training and support the structured implementation of validated interventions in the Nordic countries.
This report is the part of the new Nordic project Improving Child Health in the First 1000 Days (2025–2026), which aims to strengthen the systematic application of evidence‑based methods within social and healthcare services, and to enhance implementation expertise across the Nordic countries. The project is funded by the Nordic Council of Ministers and coordinated by Itla Children’s Foundation (Finland), in collaboration with the Nordic Network about the child’s first 1000 days – a healthy start in life.
Successful implementation is based on careful exploration and preparation
The perinatal field includes a wide range of interventions and policy frameworks that guide professionals to consider the psychosocial well-being and mental health of families within maternity and child health services (Reisenberger & Paul, 2022; World Health Organization [WHO], 2022). Effective implementation of evidence-based interventions in perinatal mental health care requires a structured, multi-level approach. Interventions become effective for families only through successful implementation. Research consistently demonstrates that weak implementation processes undermine the impact of interventions, even when strong evidence exists (Proctor et al., 2013; Nielsen, 2015; Schaefer et al., 2024; Webb et al., 2021).
The situation analysis by Daníelsdóttir & Ingudóttir (2020) identified gaps in practices. The inconsistent use of validated methods, unequal access to services, limited cross‑sectoral collaboration and insufficient evidence for many existing interventions indicate that the key challenges in the Nordic countries are not only about what services exist, but also how they are implemented. Qualitative insights from the project further demonstrate that coherent implementation structures are largely lacking across all countries (Daníelsdóttir & Ingudóttir, 2020). For this reason, the report is framed through an implementation perspective: strengthening implementation capacity is essential for ensuring that effective, evidence‑based practices are systematically adopted, scaled and sustained in real‑world services for young children and families.
A well-designed implementation process strengthens the identification of needs, supports the selection of appropriate interventions and enhances the fidelity, quality and sustainability of clinical practices, ultimately enabling intended improvements in service and clinical outcomes (Proctor et al., 2013). The EPIS Framework is a conceptual model that describes the phases of implementation: Exploration, Preparation, Implementation and Sustainment. It provides a structured way to examine the multilevel factors (organisational, relational, cultural and systemic) that shape whether and how interventions take root in practice (Aarons et al., 2011; Moullin et al., 2019). The phases of the model support coherent planning and implementation by clarifying why an intervention is needed, building the capacity for delivery, guiding its application in practice and ensuring its long-term integration (Moullin et al., 2019). The EPIS Framework describes implementation as a process unfolding across four phases:
- Exploration: assessing needs and identifying suitable interventions and contextual fit;
- Preparation: planning implementation strategies, including identifying barriers and facilitators;
- Implementation: carrying out the intervention while monitoring quality and fidelity;
- Sustainment: maintaining long-term delivery and impact.
The exploration phase involves examining the emerging or existing needs of the target group and identifying evidence-based interventions best suited to address them (Stanton et al., 2022). Evidence-based parenting interventions are essential during the perinatal period, as they have been shown to be effective and not harmful through rigorous scientific outcome evaluations (WHO, 2022). In the perinatal context, this means determining the most significant psychosocial challenges faced by families and aligning appropriate interventions with these challenges, as well as with the surrounding service system, political environment and societal conditions (Webb et al., 2021).
While this report identifies relevant needs and a range of suitable interventions, their ultimate implementation must be grounded in country- and region-specific processes to ensure contextual relevance and effectiveness. Research in perinatal health services further emphasises that implementation must account for multiple levels simultaneously: service users, professionals, organisations and broader societal norms, policies and legislation (Webb et al., 2021). The interaction between these levels shapes decisions from early interest in an intervention to its long-term sustainment. Ensuring that evidence-based practices fit both internal and external contexts, supported by explicit measures for these contextual factors, is critical for progressing from early exploration to implementation and sustainment (Moullin et al., 2019).
Without such grounding, selected practices may fail to address genuine gaps or stakeholder priorities. Although this report focuses specifically on the ‘exploration’ phase, the EPIS model provides a structure that can later be used to develop local implementation plans and to select strategies that fit the requirements of each operational context.
Aim of the report
This report is part of a Nordic project entitled Improving Child Health in the First 1000 Days (2025–2026), which is funded by the Nordic Council of Ministers and implemented by the Nordic Network about the child’s first 1000 days – a healthy start in life, together with Itla Children’s Foundation. The purpose of the project Improving Child Health in the First 1000 Days (2025–2026) is to identify current risk and protective factors, as well as existing and effective psychosocial interventions, to build an overall picture of the support available during the first 1000 days of life. The aim of this report is four-fold. It aims to:
- Update information on risk and protective factors, as well as existing and effective interventions in the countries.
- Connect information on risk and protective factors and existing, effective interventions with research on implementation in order to create a current picture of the need for support in the countries during the first 1000 days of life.
- Build a comprehensive understanding of the relevant psychosocial challenges during the perinatal period, through the identification of effective psychosocial interventions.
- Address psychosocial challenges during the perinatal period and assess where additional psychosocial interventions are needed.
This report fulfils the aim through a synthesis of three different information sources on psychosocial well-being during the perinatal period:
- First, it explores the risk and protective factors that influence the psychosocial well-being of parents and children during the perinatal period of life based on a descriptive literature review.
- Second, it maps the psychosocial interventions relevant to the perinatal period that have been evaluated and demonstrated to be effective based on a review of intervention information portals.
- Third, it collects the summary notes from Nordic expert group discussions on current phenomena and national concerns about supporting families during the first 1000 days of life.
Finally, it synthesises this information in relation to the WHO definition and conceptual framework for maternal well-being (see chapter The maternal well-being framework (WHO)). The gathered information aims to support the identification, adaptation and implementation of evidence-based interventions across the Nordic region.
Material and methods
The following section outlines the sources of information used in this report and presents the key questions guiding the analysis.
Literature review
To identify the current knowledge of the risks and protective factors, in addition to existing gaps, a literature review of meta-analyses and systematic reviews was conducted. The focus was on topics suitable for low-threshold psychosocial support and preventive approaches. Specifically, the literature review sought to answer the following question:
What are the key risk and protective factors influencing the psychosocial well-being of parents and children during the perinatal period?
The search query and inclusion criteria, together with the PRISMA flowchart, are presented in Appendices 1–2.
Inclusion criteria | Exclusion criteria |
|---|---|
The study was peer-reviewed | The study was not peer-reviewed (e.g., editorials and commentaries) |
Correct target group (parents in the perinatal period and children aged 0–24 months) | Incorrect target group |
Meta-analyses and systematic reviews from high-income countries | Other study types or studies conducted outside high‑income countries |
Articles written in English | Research articles in languages other than English |
Articles published from 2010 onwards | Articles published before 2010 |
Table 1. Inclusion and exclusion criteria in the literature review.
Certain risk factors were excluded because of their characteristics (e.g., cases managed in specialised healthcare, globally and societally exceptional periods):
- Preterm birth or low birth weight represents its own extensive research subgroup, which is treated within specialised healthcare, and was therefore excluded from this review.
- Feeding difficulties, while impactful on family well-being, also demand specialised expertise and were therefore excluded from this review.
- Adolescent motherhood was not prioritised, because it represents only approximately 0.3–1.1% of mothers in the Nordic countries (Heino & Gissler, 2024), although its prevalence and related interventions are higher in some other contexts.
- COVID-19-related studies were excluded to avoid context-specific and time-bound factors, as the review aimed to identify risk and protective factors relevant to stable healthcare and social service environments.
Mapping of psychosocial intervention information portals
Evidence-based psychosocial interventions for the perinatal period were mapped, compiled and examined in relation to identified risks. The review focused on interventions that had been rated as effective in the evaluation systems in relevant web-based information portals. The question for this review was:
Which psychosocial interventions relevant to the perinatal phase have been evaluated as effective?
The mapping was initiated by reviewing Nordic online intervention information portals and exploring the publication from the project's previous phase in 2021, i.e., The First 1000 Days in the Nordic Countries Psychosocial Interventions and Psychological Tests: A Review of the Evidence, by Martinussen and Kurki (2021). The mapping focused on online intervention portals that collect research evidence on interventions and evaluate and grade their effectiveness and are designed for professionals, with the aim of helping them make evidence-based decisions regarding the use of methods in services for children and families. The evaluation experts in the Finnish Kasvun Tuki Intervention Bank were consulted in the selection of relevant portals.
One portal for each Nordic country that had such portals was selected to review. The searches conducted in these portals mainly served as a complementary step to identify whether new Nordic interventions assessed as effective had been published after 2021. Only those interventions in the intervention information portals that provided an English language summary describing their effectiveness assessment were selected. (See inclusion and exclusion criteria in Table 2).
Inclusion criteria | Exclusion criteria |
|---|---|
The information portal was recognised and recommended by evaluation experts for the Kasvun tuki intervention bank | The information portal was not recognised and recommended by evaluation experts for the Kasvun tuki intervention bank |
The intervention was targeted at the perinatal phase, or the perinatal phase was included in the target age group | The intervention was not targeted at the perinatal phase, or did not include the perinatal phase as a target age group |
An English summary was included | No English summary was available |
Effectiveness was rated 2–4 in Nordic portals and 3–5 in the Kasvun tuki evaluation system (see Table 3) | Effectiveness was rated 0–1 in Nordic portals and 0–2 in the Kasvun tuki evaluation system |
Published by spring 2025 | Evaluation was in progress and not published by spring of 2025 (January–April) |
Information is publicly available in on-line source | Not publicly available or not in on-line source |
Table 2. Inclusion and exclusion criteria in the psychosocial intervention portal mapping.
This review was further supplemented by two British and American information portals. These were included in this review to provide a broader international perspective on interventions rated as effective. On some occasions, English-language interventions that had demonstrated effectiveness in other contexts were adapted and suggested to be introduced in a Nordic setting.
The intervention information portal review was conducted in spring of 2025, between January and April, based on information published in relevant portals. The portals used in this mapping review are introduced in Table 3. Please note that evaluations and research are ongoing, which may influence future assessments of effectiveness. The up-to-date information is recommended to be monitored through the evidence portals.
Reference | Country | Level of evidence (or grade of certainty of evidence) selected |
|---|---|---|
Nordic countries network | 2–4 | |
Kasvun tuki – Kasvun tuki Intervention bank | Finland | 3–5 |
Ungsinn – An electronic scientific journal on mental health interventions for children and young people | Norway | 2–4 |
SBU – Swedish Agency for Health Technology Assessment and Assessment of Social Services | Sweden | 2–4 (moderate–effective) |
EIF – Early Intervention Foundations, What works centre for children and families | United Kingdom | 3–4 |
NHS – Early Intervention Framework for Children and Young People's Mental Health and Well-being | United Kingdom | 3–5 |
CEBC – California Evidence-Based Clearinghouse | USA | 1–3 (reverse scale) |
USA | Model or model plus |
Table 3. Psychosocial intervention information portals and the level of evidence selection.
The checkmarks in this summary reflect what was indicated as the primary target group or objective in the portal descriptions for each intervention. For each intervention, one primary target group and one primary objective were selected based on the main focus described in the portal (see Appendices 3 and 4 for detailed information). Many interventions were found to have multiple secondary goals and effects, so additional checkmarks could apply in practice. The lists of selected psychosocial interventions, both from Nordic databases and others, are included with direct links to the web pages of each portal review (Appendices 3 and 4).
Nordic expert discussions
Nordic perinatal experts were invited during autumn 2025 to participate in national discussions based on the first summary of the findings in the scientific literature search. The representatives from each country in the Nordic network about the child’s first 1000 days invited national experts on perinatal care and support to participate in a discussion. These dialogues focused on identifying and discussing current phenomena and national concerns that require further research and solutions (identified gaps). The key points from these discussions were written down, consolidated and are presented in this report under each domain chapter. The Nordic countries participating in these discussions were Finland, Iceland, Norway and Sweden. No separate expert discussion was held in Denmark. The Danish representatives in the Nordic network have assessed that the issues raised by other experts also reflect the situation in Denmark.
The maternal well-being framework (WHO)
In the following sections, the risks and protective factors identified in the literature, the interventions identified in the database review and insights from Nordic expert discussions are categorised in relation to the WHO definition and conceptual framework for maternal well-being (Le Lez et al., 2025).
In the framework, maternal well-being is defined as “a positive state that is experienced throughout pregnancy and continuing until 1 year after the end of pregnancy, influenced by the world the woman lives in. During this dynamic and adaptive period, the woman’s partner and family receive the support, confidence and resources to thrive and realise her full potential and rights.” (Le Lez et al., 2025).
The maternal well-being framework emphases the multidomain nature of well-being and takes into account both subjective and objective well-being. Subjective well-being covers personal experiences such as the emotional state, while objective well-being encompasses external living conditions such as health, education, housing and social relationships. The framework includes six interconnected domains with subdomains that together explain the factors that shape well-being (Le Lez et al., 2025), see Figure 1.:
- The health and nutrition domain covers the conditions, background factors and measures that support the physical, mental, sexual and reproductive health of parents and children throughout their lives.
- The relationships and connectedness domain encompasses the emotional, social and interactional conditions that enable secure parent–child attachment, parental bonding, healthy couple and co‑parenting relationships, and supportive social networks.
- The security, safety and sustainable environment domain includes the structural and relational conditions that ensure safety, protection from violence and adversity, socioeconomic security and a stable living environment for families.
- The maternal autonomy, agency and resilience domain covers the psychological, social and contextual factors that enable parents to feel competent, supported, empowered and capable of managing the transition to parenthood.
- The culture and values domain encompass the cultural, linguistic, social identity-related and value-based factors that shape parental experiences, access to care, help seeking and well-being, including the needs of migrants, minority and LGBTQ families.
- The provision and experience of care domain covers the quality, accessibility, continuity and responsiveness of perinatal health and social services, and how parents experience care interactions across the pathway. It includes system-level and interpersonal factors that influence trust, safety, engagement and equitable access, as well as care models.
The framework shifts the focus of maternal well-being from preventing mortality to achieving general health and well-being. This shift of focus can facilitate equitability and sustainability (Le Lez et al., 2025).
The Nordic countries place a strong emphasis on gender equality and children’s right to care from both parents (Duvander et al., 2025). Nordic experts suggest that the maternal well-being framework could be used to analyse the well-being of both parents during the perinatal period. In the report, all findings have been synthesised according to the framework, regardless of whether they concern the mother/birthing parent or the father/non-birthing parent. For the purposes of this report, the original framework illustration has been modified to cover the well-being of both parents and caregivers and called the parental well-being framework (see Fig. 1). The Nordic expert group justified the modification by stating that, from the perspective of child development, the factors presented in the six domains of the framework affecting the ability of the adult caring for the child to ensure the child's growth and development to their full potential are not limited to the mother alone.
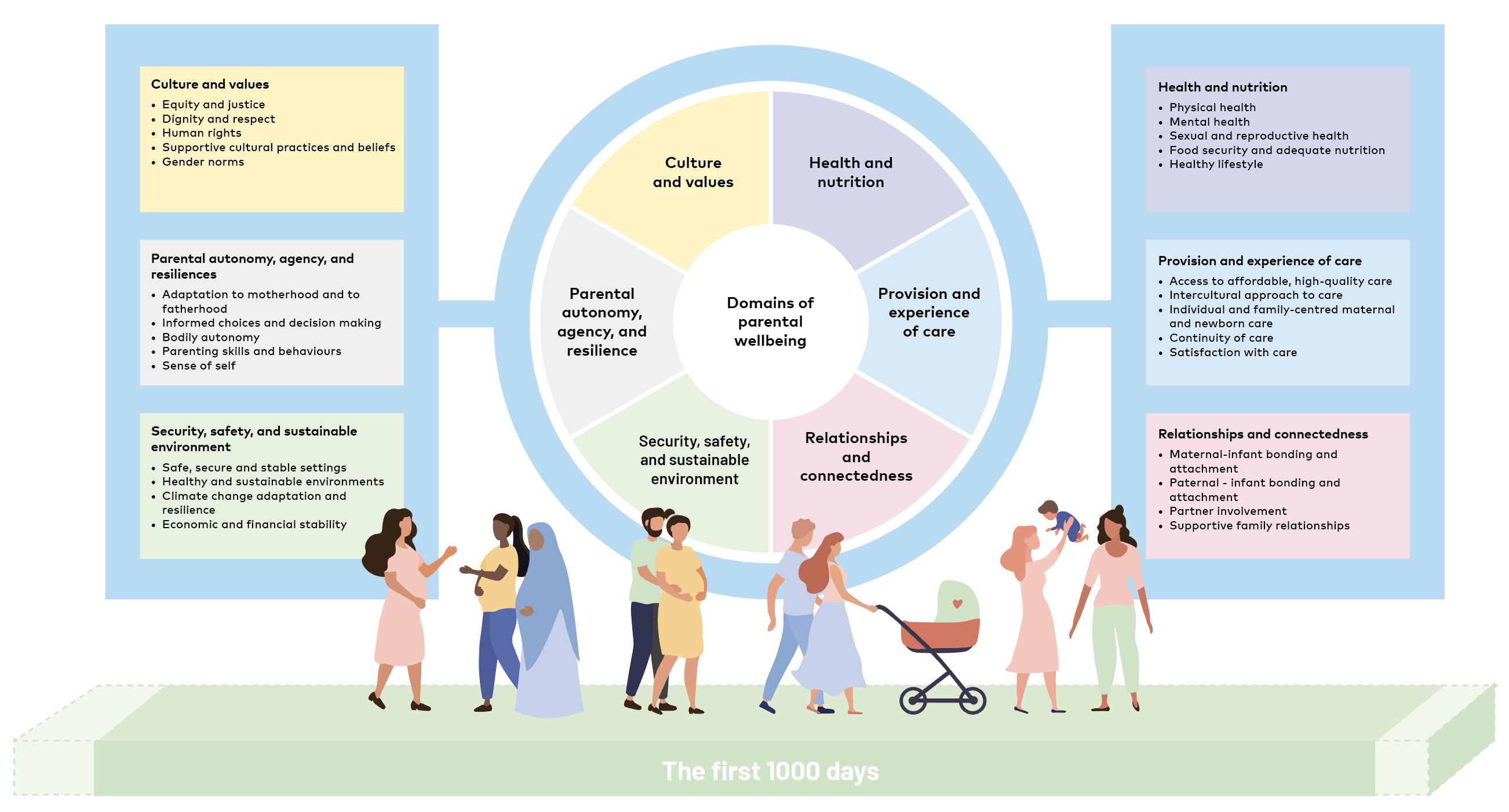
Figure 1. The parental well-being framework (adapted from Le Lez et al., 2025).
In this report, the framework was used to structure the results obtained from the literature review, the solutions that effective interventions provide and the current views of Nordic expert groups. The literature review aimed to identify which factors affect the psychosocial well-being of parents and children during the first 1000 days of a child's life. By cross-tabulating interventions assessed as impactful with risk mapping, gaps requiring solutions were identified. This was complemented with insights from national expert groups regarding the current national situation and prioritisation needs.
The maternal well-being framework builds on earlier frameworks, including the framework for child and adolescent health and well-being (WHO & UNICEF, 2023), which have been used to aid understanding of the framework and to classify factors affecting well-being. Synthesising the report’s data (literature review, intervention mapping and expert discussions) according to the framework has been somewhat challenging due to the intertwined nature of the components of psychosocial well-being their systemic interconnections. Consequently, the categorisation is inevitably a somewhat high-level overview and not entirely flawless. Nevertheless, we consider the framework to provide a valuable umbrella perspective on phenomena essential for a comprehensive examination of psychosocial well-being during the perinatal period. It is helpful in identifying gaps and developing solutions tailored to Nordic contexts.