Development of care models in the Nordic countries
Image: iStock
This chapter addresses the need to support the further development of care models for perinatal mental health in the Nordic countries. It outlines viewpoints that can inform the ongoing development efforts in the Nordic countries to develop care pathways and stepped care, and models for perinatal mental health. The perspectives presented are based on the report’s results and have been examined in light of international guidelines for perinatal mental health care and the Nordic point of view.
International guidelines for perinatal mental health care
Several international guidelines provide a shared foundation to guide the development of suggestions for comprehensive perinatal mental health service systems. Key sources include the care pathways developed by NCCMH (National Collaborating Centre for Mental Health) and RCPsych (Royal College of Psychiatrists) (NICE, 2018), the Austrian Institute for Health Technology Assessment report on perinatal care models (Reinsperger & Paul, 2022), WHO guidance on service integration (WHO, 2022) and the Australian COPE guidelines (Highet et al., 2023). Trauma-informed care has been addressed in recent systematic reviews (Benton et al., 2024; O’Brien et al., 2023).
International recommendations consistently emphasise the organisation of perinatal mental health services according to a clear and multi-tiered structure. According to these recommendations, services should form a continuum that includes universal services for all families, targeted support for risk groups and specialised services for parents with diagnosed mental health disorders (Highet et al., 2023; NICE, 2018; WHO, 2022). The overall focus is on family well-being and the quality of early parent–child interaction. Shared principles in guidelines include:
- Ensuring early identification
- Establishing integrated service pathways and clear referral routes
- Guaranteeing timely and equitable access to support
- Promoting multidisciplinary collaboration
- Applying evidence-based practices
- Adopting a family-centred approach
- Implementing a stepped care model
In a stepped-care model, support is tailored to the severity of symptoms. Screening tools such as the EPDS (Edinburgh Postnatal Depression Scale) and ANRQ (Antenatal Risk Questionnaire) are recommended for the early identification of psychological distress (Highet et al., 2023; O’Brien et al., 2023; WHO, 2022). Assessments should also include non‑birthing parents, and digital tools are encouraged to enhance accessibility and early detection.
For mild symptoms and support, guidelines emphasise psychosocial and practical interventions, including psychoeducation, guided self‑help, peer support and, where needed, home visits (Highet et al., 2023; Reinsperger & Paul, 2022). Alongside universal systems for identification and support, individualised support plans and the active involvement of the whole family are recommended. A parent’s psychological well-being strongly influences the child’s sense of safety, attachment formation and stress regulation (Highet et al., 2023). Assessing the parent–child relationship and family safety is also advised.
All guidelines stress the need for a coordinating professional, as well as sufficient staff training and supervision (Highet et al., 2023; NICE, 2018). Additional emphasis is placed on cultural sensitivity, involving experts with experience in service planning and evaluation, and the continuous monitoring of service accessibility and effectiveness (Reinsperger & Paul, 2022; WHO, 2022).
Nordic point of view
The First 1000 Days in the Nordic Countries situation analysis (Daníelsdóttir & Ingudóttir, 2020) mapped practices that support the well-being of young children and their families, including maternity and child health services and early childhood education and care. The analysis identified both strengths and areas needing development across national and regional systems.
The Nordic countries have made significant progress in systematically identifying risk factors, developing screening tools and introducing structured care models. Common priorities include early detection, family‑centred approaches and multidisciplinary collaboration. During the perinatal period, all countries screen for mental health problems, substance use, social vulnerability, relationship difficulties, interpersonal violence, traumatic experiences, young parental age and single parenthood. Child development and early interaction are also routinely monitored (Daníelsdóttir & Ingudóttir, 2020).
All countries provide more frequent visits for identified risk groups and additional follow‑up for high‑risk pregnancies, with efforts to ensure accessibility (for example, interpretation services and accommodations for disabilities). Increasing the engagement of fathers and other parents is a shared development priority (Daníelsdóttir & Ingudóttir, 2020).
Despite progress, perinatal mental health care remains underdeveloped in the Nordic countries, as well as in many countries across the European region. Common challenges are fragmented service systems, the need to strengthen cross-sectoral cooperation and gaps in services for fathers and the other parent (Danielsdóttir & Ingudóttir; Horakova et al., 2024; Reinsperger & Paul, 2022). Although all countries have general mental health policies and recommendations for the perinatal period, implementation is uneven and not always systematically monitored (Daníelsdóttir & Ingudóttir, 2020; Horakova et al., 2024).
The situation analysis also highlighted substantial variation in service availability and quality both between and within the Nordic countries, partly due to municipal autonomy and differing local resources. At best, services are well integrated and accessible; at worst, systems are fragmented, waiting lists long and costs high, particularly in rural areas and in countries where psychological treatment is not part of primary care (Danielsdóttir & Ingudóttir, 2020).
In addition to these findings, experts in the Nordic network about the child’s first 1000 days, have highlighted further nuances in how policies translate into practice, and they have expressed their concern that current access to psychological treatment during the perinatal period is more limited than six years ago, and waiting times vary considerably across service types and geographical areas.
The Nordic expert discussions emphasised the need to harmonise and clarify care pathways, particularly when parents experience more severe mental health difficulties or social risk factors. Gaps in current care pathways create delays and interruptions that undermine continuity and reduce the effectiveness of support. Early childhood psychiatric services remain limited across the Nordic countries, and significant service gaps persist. A key unmet need is access to multidisciplinary perinatal mental health teams and specialised mother–baby units for parents with moderate to severe disorders. The lack of such units often results in the separation of the mother and infant during hospital treatment, an outcome that is detrimental to bonding and recovery.
Gaps in current care pathways have been observed to contribute to delays and interruptions in support, affecting the continuity of care. Current systems identify risks but do not sufficiently provide structured preventive or specialist care. One repeatedly noted gap concerns the availability of multidisciplinary perinatal mental health teams and specialised mother–baby units for parents with moderate to severe disorders.
Nordic and Swedish studies (Hagatulah et al., 2023) further indicate that the risk of maternal suicide peaks during the first postpartum year and may also occur among women without prior specialist care, highlighting the relevance of systematic assessment. Universal and preventive services, along with consistent risk identification practices, are also viewed as important components of current systems.
Considerations for a stepped-care model in the Nordic countries
The findings indicate that maintaining the strengths of the Nordic service model (universal perinatal and child health services, systematic identification of risk groups and access to multidisciplinary support) remains important when considering the future development of care pathways. Observed gaps suggest areas where service structures may not fully align with identified needs and further development to address these gaps is needed.
This includes strengthening access to multidisciplinary perinatal mental health teams, considering the establishment of mother–baby units where they are not yet available and ensuring systematic screening and risk assessment within routine care. Supporting continuity between maternity, primary care and mental health services may also help respond to identified needs. In addition, national strategies that address training requirements, support coordinated collaboration and ensure adequate resource allocation could contribute to more consistent service provision across the Nordic context. The findings also highlight the importance of improving the implementation of evidence‑based interventions and addressing identified gaps in available psychosocial and clinical interventions, particularly in areas where effective interventions are currently limited.
Following international guidance, the proposed Nordic stepped-care model includes universal health promotion, targeted prevention for vulnerable groups, structured outpatient treatment and access to specialised units when needed.
The following section presents the proposal for a stepped-care model that may help inform the development of future care structures and care pathways in the Nordic context. The model is based on the definition proposed by Reinsberger & Paul (2022). The proposed model has been reviewed in relation to international guidelines, as well as the findings of this report. Figure 4 summarises the components of this model and illustrates how they could be considered when developing stepped-care approaches in the Nordic countries.
The proposal for a stepped-care model
Universal level (for all families):
Psychoeducation and support for preparing for parenthood
- Child development and needs
- Transition to parenthood and parent relationship
- Parenting skills and basic care of the infant
- Support for parents' own coping strategies and resilience
- Special attention to fathers and other parents
- Awareness of mental health challenges during the period
- Language-specific information and use of interpretation services
Timely identification and discussion
- Maintain universal identification through structured and consistent screening for anxiety and stress, as well as depression screening with validated and language-specific tools
- Follow screening with structured follow-up conversations, clear referral pathways and timely appointments, as needed
- Confidential screening for intimate partner violence and referral to safe services
Adequate and respectful support during pregnancy, childbirth and breastfeeding
Peer support
Targeted preventive support for high-risk groups or care for parents with mild symptoms:
Identify high-risk groups
- Structured psychosocial assessment to identify high-risk families
- Pre-pregnancy counselling for high-risk families
- Home visits to reinforce early support
Supportive counselling in maternity clinics and rapid psychological support for parents
Guaranteed access to evidence-based and effective psychosocial care
- Systematic implementation of interventions with research evidence meeting identified risks
- Digital interventions
- Targeted interventions
- Group or community-based interventions
- Culturally appropriate and language-specific interventions
Monitoring and support for early interaction
Support after pregnancy loss, negative or traumatic childbirth, child health-related worries
Care and support for parents with multiple risks and moderate symptoms:
Care coordinated by a multiprofessional perinatal mental health team
- Including psychiatric, psychological and social service expertise
- Individualised support plans
- Assessment of suicide risk whenever symptoms are present and rapid escalation to perinatal psychiatric expertise
Psychotherapeutic or targeted interventions
Early interaction monitoring and support
Specialised care for parents with severe psychiatric symptoms:
Specialised perinatal mental health services
- Outreach services
- Individualised support plans
- Support for family members
- Assessment of child protection needs (all children in the family)
Mother–baby units where the mother and child can stay together during hospitalisation
Acute crises:
Immediate assessment (e.g. postpartum psychosis, serious risk of suicide)
Rapid referral to perinatal psychiatric expertise
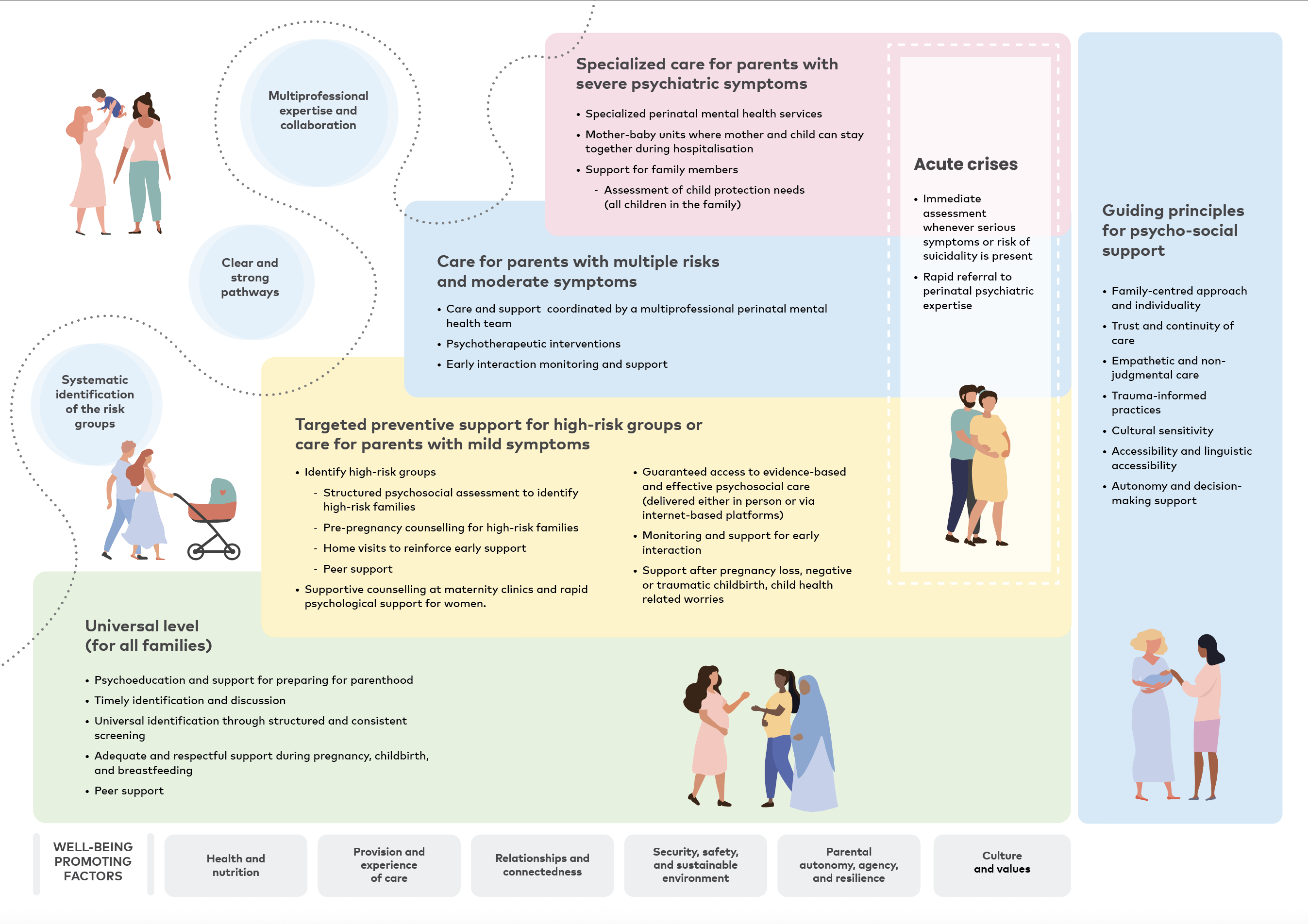
Figure 4. Proposal for a stepped-care model.
Guiding principles for psychosocial support
Evidence indicates that the quality of encounters and interaction with parents, together with individual and cultural factors, have a significant impact on later mental health. Negative experiences are associated with poorer well-being, while positive experiences protect mental health. Early identification of support needs during the transition to parenthood is a cost‑effective way to promote mental health. Families facing cumulative risks are particularly dependent on timely, appropriate support including individualised care, confidential communication and cultural sensitivity.
The following section presents the principles that, based on the material of this report, strengthen the ability of services to meet the psychosocial support needs of families during the first 1000 days and support the implementation of a stepped‑care model.
Family-centred approach and individuality
Treatment should be built around individual needs and the well-being of the whole family. International guidelines emphasise the importance of involving the whole family in care. The pregnant or postpartum parent together with the infant is at the centre of care, but the needs of fathers and other possible siblings for support should also be considered. Mental health challenges can strain relationships and family dynamics and increase the risk of isolation. Family-centred care strengthens resilience, the sense of security and the healthy development of the child.
Trust and continuity of care
The quality of care received, and the experiences of care emerged as among the significant factors affecting mental health. A trusting therapeutic relationship and continuity of care, together with good interaction, are key protective factors for mental health. International guidelines emphasise the continuity of care through structural solutions such as integrated care pathways, the appointment of a coordinating professional and multidisciplinary collaboration.
Empathetic and non-judgmental care
International guidelines emphasise that care should respect individual values, be culturally sensitive and be based on interactions that promote safety. Empathetic, non-judgmental care is a key principle supported by international recommendations through a trauma-informed and family-centred approach. Sensitive interaction reduces stigma, encourages help-seeking and protects mental health. Consistent guidance and a non-judgmental environment strengthen parental confidence.
Trauma-informed practices
Trauma-informed practices build a sense of safety and reduce the risk of re-traumatisation. They also protect mental health and strengthen autonomy. This requires sensitive communication, opportunities for decision-making and structural measures such as staff training and guidance. In addition, trauma-informed and culturally sensitive care and continuous assessment support trust and prevent the discontinuation of care.
Cultural sensitivity
Culturally sensitive care ensures equality and trust. This includes interpretation services, plain language information and training for professionals on cultural differences. Cultural competence prevents misunderstandings and discrimination and is particularly important for immigrants and other vulnerable groups. International guidelines also emphasise structural measures, such as systematic training and guidance for staff.
Accessibility and linguistic accessibility
Services must be physically accessible and offer linguistic accessibility. This means interpretation, plain language materials and staff training on accessibility. Accessibility promotes participation and prevents the discontinuation of care.
Autonomy and decision-making support
Parental autonomy and decision-making should be ensured in all stages of care. This strengthens their sense of control and reduces fears associated with stigma. Clear information and decision-making support are particularly important for parents with cognitive challenges. Autonomy is supported by culturally appropriate practices and a confidential care relationship.
Guiding principles for psycho-social support
- Family-centred approach and individuality
- Trust and continuity of care
- Empathetic and non-judgmental care
- Trauma-informed practices
- Cultural sensitivity
- Accessibility and linguistic accessibility
- Autonomy and decision-making support
Next steps
While the report outlines common challenges and opportunities for the Nordic countries, national differences must be acknowledged. Each country operates within its own legislation, service structures and demographic conditions. Implementing coherent care pathways therefore requires assessing the suitability of existing structures and interventions at national and regional levels. Workforce training and policy measures are also needed to support sustainable implementation. Because of these contextual differences, the findings cannot be applied uniformly. Below are some suggested steps and measures that could be taken at the Nordic, national and regional levels to translate the Nordic-level insights into national contexts:
Nordic level
- The model should support the selection of interventions that are suitable for high-risk groups.
- The model should strengthen systematic, cross‑country research on intervention effectiveness, enabling the identification of evidence gaps and ensuring that the needs of minority and high‑risk groups are addressed.
- Develop joint training modules on perinatal mental health and early interaction support.
- Establish regular Nordic knowledge-sharing forums to disseminate implementation experiences and good practices across countries.
National level
- Assess national capacity and readiness by reviewing identified needs and intervention gaps in relation to legislation, service models and available resources.
- Support the systematic implementation of interventions found effective in the Nordic context by establishing national frameworks, funding structures and training programmes that enable consistent adoption across service settings.
- Develop culturally sensitive and accessible services for parents with disabilities, sexual and gender minorities and immigrant families and assess equity implications.
- Develop national training programmes on perinatal mental health and early interaction support.
Regional level
- Conduct local context analyses to identify obstacles and enablers and ensure staff training and practical implementation planning to embed interventions to regional service structures.
- Ensure systematic screening of risk factors for all parents, including fathers and non-birthing parents.
- Support peer support groups and community‑based models, including father groups and family coaching.
- Strengthen attention in services to cultural and linguistic accessibility for migrant, minority and indigenous families.
These steps and measures will help countries progress from the exploration phase to the preparation phase of the EPIS Framework previously mentioned (see chapter Successful implementation is based on careful exploration and preparation), which includes adaptation, detailed planning and stakeholder engagement. Future development should prioritise building consistent care pathways and implementation processes that support this stepwise model, thereby strengthening effectiveness, equity and long‑term improvement in perinatal services. The selection of interventions integrated in stepped-care models should balance effectiveness and suitability, considering cultural relevance, resource requirements and organisational capacity. A shared Nordic assessment framework would support collective understanding of suitability and help identify common solutions to shared challenges.
The current report provides a foundation for the exploration phase of implementation by identifying key psychosocial needs and risk factors for parents and children, reviewing existing interventions from both Nordic and international sources, and collating international guidelines alongside Nordic expert dialogue findings. Together, this establishes the evidence base needed to move toward the preparation and implementation of contextually appropriate support across the Nordic region. The report highlights gaps between evidence and practice and points to some shortcomings in the implementation structures. It acknowledges equity considerations and the complexity of contextual factors, and emphasises the need for cross-country collaboration and resource pooling to strengthen implementation efforts across the region. A coordinated Nordic approach can provide a strong basis for improving service equity, strengthening quality and supporting sustainable, context‑sensitive implementation for young children and their families.