Appendices
Appendix 1. Search query
P= pregnan* OR "pre-nat*" OR prenat* OR prepart* OR "ante-nat*" OR antenat* OR "ante-part*" OR antepart* OR "peri-nat*" OR perinat* OR "peri-part*" OR peripart* OR puerper* OR "post-nat*" OR postnat* OR "post-part*" OR postpart* OR mother* OR maternal OR father* OR paternal OR infan* OR newborn OR neonat* OR baby OR babies OR antepartum OR antenatal OR "expecting mother" OR "expecting parent" OR infant
C= "anxiety disorder*" OR "depression" OR "adjustment disorder*" OR "tokophobia" OR "fear of childbirth" OR "eating disorder*" OR "substance use disorder*" OR "alcohol use disorder*" OR "alcoholism" OR "drug abuse" OR "bipolar disorder*" OR "schizophrenia" OR "psychotic disorder*" OR "psychosis" OR "psychotic" OR "traumatic childbirth" OR "post-traumatic stress disorder" OR "PTSD" OR "suicidality" OR "suicidal ideation" OR "self-harm" OR "loneliness" OR "poverty" OR "homelessness" OR "low educational level" OR "low education" OR "unemployment" OR "financial insecurity" OR "domestic violence" OR "intimate partner violence" OR "relationship problem*" OR "divorce" OR "separation" OR "family conflict*" OR "lack of social support" OR "pregnancy complication*" OR "preterm birth" OR "adverse childhood experience*" OR "psychological stress*" OR "psychological distress*" OR "psychosocial distress" OR "psychosocial stress*" OR "sleep problem*" OR trauma* OR phobia* OR "obsessive compulsiv*" OR "social problem*" OR "social support" OR "coping mechanism*" OR "protective factor*" OR "risk factor*" OR "resilience" OR "positive self-image" OR "acceptance of life changes" OR "partner support" OR "family support" OR "community support" OR "peer support" OR "doula support" OR "stable living environment" OR "responsiveness to infant needs" OR "positive parenting beliefs" OR "knowledge about pregnancy" OR "mental health" OR attachment" OR "bonding" OR "connection" OR "relationship" OR "interaction" OR "early
interaction" OR "mother baby interaction" OR "father baby interaction"
interaction" OR "mother baby interaction" OR "father baby interaction"
C= "healthcare" OR "maternity care" OR "perinatal care" OR "health services" OR "obstetric care" OR "public support" OR "community support" OR "government support" OR "welfare programs" OR "social services" OR "family support services" OR "child welfare services" OR "mental health services" OR "counselling services"
Additional filters
NOT= "teen pregnancy" OR "adolescent pregnancy" OR "young mothers" OR "teen mothers" OR "adolescent mother*" OR "breastfeeding" OR "infant nutrition" OR "infant feeding" OR "formula feeding" OR "complementary feeding" OR "COVID-19" OR "SARS-CoV-2" OR "pandemic" OR "coronavirus" OR "allerg*" OR diabet* OR "scoping review" OR "umbrella review" OR "oral health" OR "sexual and reproductive health" OR haematolog* OR hemorrhage* OR "obstetric fistula" OR "HIV" OR africa* OR "sub-sahara*" OR india* OR "low- and middle-income countr*"
Additionally, the search was limited to systematic reviews and meta-analyses at the abstract, title, and keyword levels. Further restrictions included the English language and the years 2010–2025.
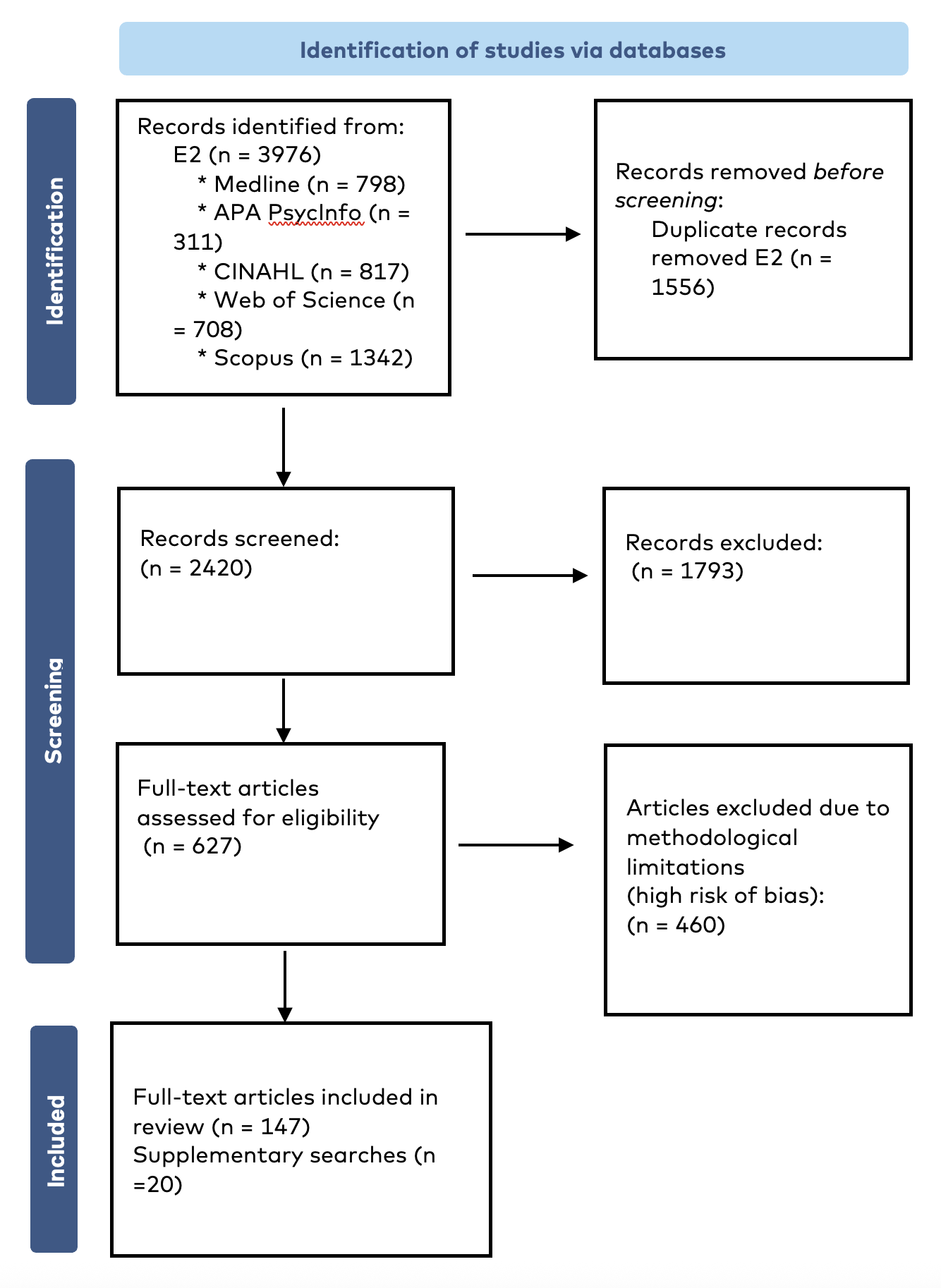
Appendix 2. PRISMA flow chart
Appendix 3. Psychosocial intervention with effectiveness grading (Nordic portals)
Intervention | Population | Goal | Classification | Summary | Outcome | Effectiveness grading* |
Attachment and Behavioral Catch-Up (ABC) | Parents (biological or foster) of children aged 6–24 months who have experienced adverse events such as abuse or neglect. | To support parents in providing care when the child is stressed and in preventing harmful reactions. Attachment-based. | Targeted at a risk group | Ten weekly home visits, attachment-based therapy, each lasting 60–90 minutes, incorporating video-based exercises and coach feedback. | Improvements in children's attachment security, stress regulation (cortisol levels), emotion regulation and social-emotional competence. | Nordic review 3/4 (Incl. Nordic studies) |
CBT | Mothers experiencing perinatal depression | To reduce depressive symptoms | Therapeutic intervention | Sessions that focus on psychoeducation, cognitive restructuring, behavioural techniques, exposure therapy and stress management. CBT includes integration of planning and support for the postpartum needs whilst the patient receives treatment in the antenatal period. | In non-psychotic perinatal mental health disorders, CBT has been shown to effectively reduce symptoms of anxiety, stress and depression, and reduce depression diagnoses post-treatment and on follow-up. | SBU Moderate (2022) |
Child–Parent Psychotherapy (CPP) | Children aged 0–5 years who have experienced or witnessed a traumatic event and are exhibiting attachment, behavioural or emotional difficulties as a result, together with their parents. | To support and strengthen the relationship between a child and his or her caregiver as a vehicle for restoring the child's cognitive, behavioural and social functioning | Therapeutic intervention | Psychodynamic-oriented treatment and interpretation during play is one of the main techniques. Takes one year to complete and consists of therapist meetings with the child and parent on a weekly basis. | Effects: children’s and mothers’ traumatic stress symptoms, children’s internalising and externalising symptoms and mothers’ bias toward their children’s fearful faces. | Nordic review 2/4 (Incl. Nordic studies) |
COPEing with Toddler Behavior (CWTB) | Parents of toddlers (1–3 years) who have behavioural problems (reported by parents) | To improve parent–child interaction and prevent the development of disruptive behaviour disorders. | Targeted at a risk group | Eight-session parent training programme focusing on effective parenting styles and strategies for toddlers, using an active learning model. Group therapy | Significant effects on several primary and secondary outcomes in the CWTB group compared to the control group (e.g., child behaviour problems, positive parent–child interaction and parental over-reactivity). | Nordic review 2/4 (No Nordic studies) |
Family checkup (FCU) component 1-24months | The Family Check-Up (FCU) is empirically validated for families of children age 2–17 years, with components for children aged 1–24 months with multiple needs: Socioeconomic challenges Mental health concerns (e.g., depression, stress) Limited parenting support or skills Early signs of child developmental or behavioural concerns | To support healthy development and strengthen the caregiver–child relationship. | Targeted at a risk group | Delivered directly to individual families in 3 key stages, composed of an initial Interview, followed by assessments and conclusions, with feedback to parents about strengths and challenges. The programme’s strengths-based, collaborative approach threads through each of these meetings, usually conducted once a week over three consecutive weeks. | Significant reduction in child behavioural difficulties and significant improvement in caregiver positive behavioural support | Nordic review 2/4 (Incl. Nordic studies) |
ICDP | Parents of children aged 0–18 years, including expectant parents, as well as professionals working with children, young people and families | To enhance positive interaction between a parent or other caregiver and a child. This is achieved by strengthening the caregiver’s sensitivity to notice and recognise the child’s needs and initiatives. | Universal prevention (also adapted for specific risk groups) | Implemented for parents as group guidance, individual guidance or a combination of both. The guidance can be provided, for example, in connection with early childhood education and maternity and in child health clinics | The programme was found to have statistically significant positive effects specifically on parental self-efficacy and emotional sensitivity | 4/5 Kasvun Tuki (2024) (Incl. Nordic studies) |
Incredible Years® (IY) – Parents and Babies Program + Toddler Basic Program | Parents of infants (0–1 year). | To support parent–child attachment and promote the child’s physical, cognitive and emotional development. | Universal prevention (adapted versions for specific risk groups and treatment) | Group-based guidance using videos, discussions and exercises. Focused on infant development, creating a safe environment and strengthening the parent’s role. | Improved attachment security, parental self-efficacy and child development | Nordic review 2/4 (Incl. Nordic studies) |
IPT (interpersonal therapy) + IPTG (group) | Mothers with depressive symptoms (pre-/peri-/post-natal) | To alleviate symptoms of depression and other mental health disorders by empowering isolated individuals to improve their relationships and social support networks | Therapeutic intervention | 12–16-week symptom-targeted, structured intervention. Specific strategies to deal with whichever of the four potential problem areas is the focus | Fewer cases of depression, significantly greater decrease in depressive symptoms, postpartum adjustment and social adjustment, increase in positive involvement with the child | Nordic review 3/4 (Incl. Nordic studies) |
Mamma-Mia | Universal and risk factors for postpartum depression | To support preparation for parenthood: psychoeducation, emotional skills and cognitive-behavioural strategies | Universal prevention | Web-based, to support preparation for parenthood: psychoeducation, emotional skills, and cognitive-behavioural strategies | Reduction in depressive symptoms and improvement in the mother's psychological well-being. | Nordic review 3/4 (Incl. Nordic studies) |
Marte Meo | Parents of the youngest children, first-time mothers, vulnerable or insecure mothers | Preventing maternal stress, increasing sensitivity and confidence | Targeted at a risk group | Video-based intervention for promoting child development. The videos are used by the therapist to observe what happens in the interaction between the parents and their children, for mapping the children’s needs and in parent supervision. | Better interaction, maternal sensitivity, maternal confidence and less maternal stress | Nordic review 2/4 (Incl. Nordic studies) |
Mellow Bumps (MB) | Pregnant mothers experiencing stress or mental health problems such as depression, additional social care needs | To decrease stress in expectant mothers, improve their understanding of their infant's social-interactive capacity, and promote a nurturing relationship | Targeted at a risk group | Group therapy focuses on emotions related to motherhood, stress management and understanding the infant’s capacities. | Reduction in maternal stress levels and better preparation for motherhood | Nordic review 2/4 (No Nordic studies) |
Minding the Baby® (MTB) | First-time pregnant women aged 14–25 years with a high risk of multiple social factors | To improve socioemotional outcomes, strengthen the secure bond between the mother and infant, and enhance the ability to respond to the child's needs, overall parenting skills. Attachment-based | Targeted at a risk group | Home visits, attachment-based, beginning in the second trimester of pregnancy and continuing through the child's first year of life. The goal is to teach protective skills and emotional regulation. | Aims to improve child and maternal socioemotional outcomes: Positive effects on parental sensitivity, the child's physical and psychological development, and overall family resilience | Nordic review 3/4 (3 /EIF) (Incl. Nordic studies) |
Modified Mother–Infant Transaction Program (MITP) | Preterm infants and their parents | For preterm infants: the programme aims to enhance parental understanding of the infant’s cues and promote sensitive and consistent responses, supporting the child’s healthy development. | Targeted at a risk group | Home visits that guide parents in recognising infant cues and engaging in responsive interactions. The programme focuses on strengthening child development and family relationships. | Positive effects on parental sensitivity, quality of interaction and the infant’s cognitive and social development | Nordic review 4/4 (Incl. Nordic studies) |
Neonatal Behavioral Assessment Scale (NBAS) | Infants (0–2 months) and their parents. | To sensitise parents to infants’ capacities and individuality, and enhance the parent–infant interaction and relationship | Universal prevention | Improving caregiver–infant interaction at the behavioural level through a specific focus on caregiver responsiveness during the earliest days and months of the infant's life | Strengthened interaction between the caregiver and infant | Nordic review 2/4 (No Nordic studies) |
Newborn Behavioral Observation (NBO) | Infants (0–3 months) and their parents. | Preventive support for early parent–infant interaction: to improve parents' awareness of their infant's competencies and thereby promote better interaction. | Universal prevention (also adapted for specific risk groups) | The intervention aims to improve parents' awareness of their infant's competencies and thereby promote better interaction. Clinicians video record the interaction and use the recordings in supervision. Home-based. | The intervention is based around the child, with parents focusing on how the child is communicating with them, and how the parents understand their child. | Nordic review 2/4 (Incl. Nordic studies) |
Newborn Individualised Developmental Care and Assessment Program (NIDCAP) | Preterm infants/ infants with very low birth weight admitted to a newborn/ neonatal intensive care unit (NICU), together with their parents. | Promoting healthy development, emotional bonding and empowerment | Targeted at a risk group | Sequential, formalised, naturalistic observations of the infant prior to, during and after caregiving procedures. | Positive effects on cognitive and motor development improve long-term neuro-developmental or short-term medical outcomes. | Nordic review 2/4 (Incl. Nordic studies) |
Nurse–Family Partnership (NFP) | Young first-time mothers, especially families with a low socioeconomic status | Better pregnancy outcomes, improved child health and development, increased economic self-sufficiency | Targeted at a risk group | A home-visit-based programme in which trained nurses support the family. | Positive effects on the child’s health, the mother’s self-esteem and the family’s well-being. | Nordic review 3/4 (Incl. Nordic studies) |
Nurture and Play | Mothers with depression | To strengthen the emotional bond between the parent and child by enhancing parental sensitivity, responsiveness and playfulness through attachment-based interactions. | Targeted at a risk group | Group-based guidance involving interactive exercises and play. Includes activities that help mothers understand their child’s signals and emotions. | Reduction in depressive symptoms and improved interaction with the child. | Nordic review 2/4 (Incl. Nordic studies) |
Nyyttigroup | Pregnant mothers with fear of childbirth | Supporting first-time mothers in alleviating childbirth fear and strengthening their readiness for birth and parenthood | Targeted at a risk group | A semi-structured peer group-based intervention, targeted at pregnant mothers expecting their first child. The intervention is based on strengthening body awareness and self-regulation, with peer groups as well as instructive and educative ways of working (psychoeducation) | Preparedness for childbirth increased among mothers who gave birth to their first child in the intervention group. With a reduced fear of childbirth, motherhood strengthened in mothers who participated in the Nyytti group (Finland) | 2/3 Kasvun Tuki (Incl. Nordic studies) (2021) |
Parent–Baby Intervention | Parents with depression and other mental disorders, and their babies (0–1 years). | The aims of the intervention are to strengthen social interaction and contact with the infant. | Therapeutic intervention | The aims of the intervention are to strengthen social interaction and contact with the infant and to reduce the risk of future socio-emotional problems in the child. 8–10 home visits every 1–2 weeks. During each home visit, the home visitor monitors and videorecords the parents and children during everyday activities, such as bathing or feeding the baby. | Positive effect on the quality of the mother–infant interaction, better infant attachment security and social competence | Nordic review 2/4 (No Nordic studies) |
Parent–Child Interaction Therapy (PCIT) | Families with behavioural problems or difficulties in stress regulation | To strengthen the parent–child relationship, reduce disruptive behaviours in children and empower parents with effective strategies for managing their child's behaviour | Therapeutic intervention | Individual sessions using real-time coaching, where the parent interacts with their child and receives feedback from a coach through an earpiece. The exercises focus on reinforcing positive behaviour and setting boundaries | Significant improvements in child behaviour, parental stress levels and parenting techniques | Nordic review 4/4 (Incl. Nordic studies) |
Parent–infant psychotherapy (PIP) | Parents of infants aged 24 months or younger who have problems in parent–infant relationships, problems with theinfant’s excessive crying and sleeping/eating difficulties | To strengthen the parent–child relationship and promote healthy attachment | Therapeutic intervention | A parent–infant psychotherapist works directly with the parent(s) and infant | Effects: favourable outcomes over time for the PIP-treated dyads relative to the control group on several measures of maternal mental health, parenting stress and parental representations of the infant and their relationship. | Nordic review 2/4 (Incl. Nordic studies) |
Safe Environment for Every Kid (SEEK) | Families with a risk of abuse or neglect towards the infant | To help prevent child abuse and neglect | Early prevention for risk groups | Based on integrating child healthcare to identify and prevent domestic violence and parental stress. | Reduction in cases of abuse and improvement in family well-being | Nordic review 2/4 (Incl. Nordic studies) |
Supporting Parent–Child Interaction | 0–18-month-old children and their parents | The intervention is primarily intended to support pregnant and post-natal women and young children, and employees working with their families. | Universal prevention | The interview is conducted at home, with both parents present. It is recommended that the interviews should take place during the last trimester at the latest, and within 4–8 weeks after delivery. | Mothers were more responsive towards their children, provided more appropriate play material, were more involved and used less control than mothers in the control group | Nordic review 2/4 (Incl. Nordic studies) |
Transdiagnostic Cognitive Behavioral Group Treatment (TCBGT) for Pregnant Women | Pregnant women with mild to moderate symptoms of depression or anxiety. | To reduce symptoms of anxiety and depression during and after pregnancy | Therapeutic intervention | Cognitive-behavioural group therapy focuses on emotion regulation, challenging thought patterns and stress management. | A significant reduction in symptoms of depression and anxiety. | Nordic review 2/4 (Incl. Nordic studies) |
Triple P – Positive Parenting Program® (Triple P for Baby) | Parents of young children (0–2 years), although the programme can be adapted for other age groups. | To support parenting and promote child development. To prevent behavioural and emotional problems in the children–baby version: prenatal and post-natal parents interested in learning about baby development and behaviour | Universal prevention | A multi-level programme that may include individual sessions, group meetings or self-directed learning. Triple P for Baby is an individual and group-based intervention aimed at prenatal and postnatal parents interested in learning about baby development and behaviour, common changes when their baby arrives, as well as strategies to help teach their baby new skills and behaviours. There is also a Triple Discussion Group version. | Reduction in children's behavioural problems and improvement in parenting skills | Nordic review 3/4 (Incl. Nordic studies) |
Video Interaction Guidance (VIG) | Parents and children, especially experiencing challenges in early interaction. | Promotes attunement, sensitivity and mentalisation in relationships. | Universal prevention | Video recordings of parent–child interactions are used. Video clips are sanalyssed together with a coach. VIG can be used in various contexts | Improvement in parental sensitivity and increased emotional security for the child | Nordic review 2/4 (No Nordic studies) |
Watch, Wait and Wonder | Children and parents, especially families experiencing problems related to interaction | Strengthening of attachment and improvement in the child’s self-regulation | Targeted at a risk group | An intervention in which the parent observes their child’s spontaneous behaviour and responds to it. The interaction situations are sanalyssed in discussion with a therapist. | Strengthening of attachment and improvement in the child’s self-regulation | Nordic review 2/4 (No Nordic studies) |
Appendix 4. Psychosocial intervention with effectiveness grading (British and American portals)
Intervention | Population | Goal | Classification | Summary | Outcome |
IPP Infant-parent psychotherapy | Mothers identified as being depressed, anxious, traumatised or at risk of maltreating their child. | To strengthen the parent–infant bond by addressing parental trauma and insecurities to prevent insecure attachment and support healthy infant development | Therapeutic intervention | A psychoanalytic intervention targeting mother–infant dyads who may be at risk of an insecure attachment. To prevent insecure attachment or to shift an insecure to a secure attachment, as measured by Ainsworth’s Strange Situation. Mothers attend weekly sessions at home with their infant (< six months) for a period of 12 months or longer. | Supports children's mental health and well-being (specified) |
Adolescent Parenting Program (APP) | First-time pregnant and parenting youths aged 12 to 19 years old, and who must be enrolled in school or a GED completion programme | Supporting young first-time mothers to prevent a repeat pregnancy, complete their high school education, acquire job skills and improve their parenting skills | Targeted at a risk group | Participants in the programme receive monthly home visits using either the Partners for a Healthy Baby or Parents as Teachers home-visiting curriculum, along with 24 hours of prescriptive group education with their peers. | Helps mothers become self-sufficient and better able to support themselves and their families. It also establishes a strong, stable foundation upon which their child will be raised. |
Child First | Mothers of children at risk of emotional problems, developmental delay, abuse and neglect (version for toddlers) | To provide a tailored package of support to meet the unique needs of each family. | Targeted at a risk group | Bridge universal, targeted and specialist/intensive services to provide a tailored package of support to meet the unique needs of each family. Comprehensive needs assessment of each family’s specific strengths and weaknesses. Motivational interviewing is used during these first visits to actively engage and recruit parents to the programme; weekly home visits begin for a period of 6 to 12 months. | Reduced psychiatric symptoms in parents, reduction in child externalising difficulties |
Computer-Assisted Motivational Intervention (CAMI) | Pregnant and/or first-time parenting adolescents aged 18 and younger | To help adolescent mothers make healthier choices to reduce their risk of repeat pregnancies and sexually transmitted infections | Targeted at a risk group | CAMI consists of 60-minute sessions conducted in two parts by trained counsellors who meet one-on-one with pregnant and/or parenting adolescent mothers, aged 12 to 18 years. | Preventing repeat pregnancies and staying healthy |
EPEC Baby and Us –version (parents of babies 0-1) | Families living in areas of high social deprivation and their aims centre on improving the parent–child relationship, prevention of later child behaviour difficulties and increasing parental confidence. | To increase parenting skills and confidence, preventing later child behaviour difficulties. | Targeted at a risk group | A group parenting intervention, delivered by parents who have previously participated in a parenting group and have undertaken the ten-week EPEC training programme for peer facilitation | Improvements in children’s externalising behaviours. Effects on positive parenting and impact on parenting stress. |
Family Foundations (FF) (eFF) | Couples expecting their first child, delivered at any time during the mother’s pregnancy. | To enhance parenting skills such as communication, conflict resolution, sharing duties, supporting child development. | Universal prevention | The programme is delivered by male and female co-facilitators with a QCF-level 6 in a helping profession. Parents attend five weekly sessions in which they learn strategies for enhancing their communication, conflict resolution and the sharing of childcare duties. Couples return for four more weekly sessions, two to six months after the infant is born, to learn strategies for communicating effectively as parents and supporting their child’s development | Reduced adverse birth outcomes; improvements in infant soothing ability, attention sleep and child social–emotional functioning. |
Family Growth Center, The (FGC) | Adolescent mothers aged 13–17 years and their infants from birth to 2 years of age in high-risk neighbourhoods | Improved access to a comprehensive set of educational and support services within their own high-risk neighbourhood | Targeted at a risk group | A community-based family support programme designed to reduce repeat pregnancy and school drop-out rates among adolescent mothers. The programme aims to provide teen mothers in high-risk neighbourhoods with a comprehensive set of educational and support services, offered within family and neighbourhood contexts. | Reduced school dropouts and finding support services |
Family Nurse Partnership | Young mothers expecting their first child. | To learn about their young child’s health and development and receive support for their own well-being. | Targeted at a risk group | Mothers enrol in the programme early in their pregnancy and receive visits from a family nurse on a weekly basis before and for the first six weeks after the birth of their child. Visits then continue fortnightly until three months before the child’s second birthday, when visits become monthly in preparation for the programme ending. 64 visits in total are scheduled. During these visits, mothers learn about their young child’s health and development, and receive support for their own well-being. | Prevention of obesity and promotion of healthy physical development |
Family Spirit® | Any at-risk or young adult mother (under 25 years of age) who is pregnant (ideally 28 weeks of gestation or earlier) and/or has a child younger than 3 years old and lives in a Native American community; can be used regardless of ethnicity | To increase parenting knowledge and skills | Targeted at a risk group | A culturally tailored home-visiting programme designed to promote optimal health and well-being for parents and their children. Family Spirit combines the use of paraprofessionals from the community as home visitors and a culturally informed, strength-based curriculum as a core strategy to support young families. Parents are given information and taught skills designed to promote healthy development and positive lifestyles for themselves and their children. | Increase in parenting knowledge and skills Decrease in psychosocial risks that could interfere with positive child-rearing. Increase in familiarity with and use of community services that address specific needs Increase in life skills and behavioural outcomes across the lifespan |
Mellow babies | Mothers (and fathers run separately) with babies aged 0–12 months with multiple indicators of developmental risk. | To increase positive parent–infant interactions; reduce negative parent–infant interactions; improve infant development, including language development; reduce child protection concerns; and improve adult well-being | Targeted at a risk group | This programme is delivered over 14 weekly sessions for an afternoon’s duration following on from Mellow Mums or Mellow Dads and an interactive lunch for parents and babies. | Improvement in child behaviour/conduct problems post-intervention. Improvement in maternal mental health and parenting confidence, reduction in mothers' depressed mood and increase in positive interactions between mothers and infants. Mothers with partners experienced greater benefits in mental health and parenting confidence compared to single mothers. |
Michigan Model of Infant Mental Health Home Visiting, The (IMH-HV) | Families, specifically parents and their infants/toddlers ages 0 (during pregnancy) to 36 months, who present challenges to the parent–child relationship | Aims to increase parental competencies, promote mental health and sensitive caregiving, and thus reduce risks for the infant/toddler and lessen the probability of intergenerational transmission of the effects of unresolved loss and trauma in parents. | Targeted at a risk group | A needs-driven, relationship-focused intervention for parents and infants/toddlers aged 0 (pregnancy) to 36 months. IMH-HV aims to meet the needs of families at risk of relationship problems, child abuse and/or neglect and behavioural health concerns. | Increase in parental competencies, promotion of mental health and sensitive caregiving, and thus reduction in risks for the infant/toddler and lessening of the probability of intergenerational transmission of the effects of unresolved loss and trauma in parents. |
Mom Power® | Mothers (e.g., biological, adoptive, foster, etc.) of child(ren) aged 0 (during pregnancy) to 6 years, where the mothers are experiencing adversity, have past experiences of trauma or abuse, and/or current mental health challenges (e.g., posttraumatic stress and/or depressive symptoms) | To reduce maternal depression and post-traumatic stress symptoms, parenting stress and increase the sense of parenting competence To secure safe attachments for the child. Also aims to reduce isolation and build social networks | Targeted at a risk group | An integrated mental health and attachment-based parenting programme that incorporates a manualised intervention delivered by 2 facilitators across 13 sessions (3 individual and 10 group sessions), with corresponding parent and child group curricula. | The programme seeks to nurture resilience through strengthening protective factors, improving mental health and promoting sensitivity and responsive parenting. |
Parent-Child Assistance Program (PCAP) | Pregnant or parenting mothers (up to 12 months postpartum) who have alcohol and/or drug use disorders and their children aged 0 to 3 years. | To obtain treatment for alcohol and drug use and remain in recovery, using community resources | Targeted at a risk group | Serves high-risk mothers with substance use disorders and their families using a theory-based model (relational theory, stages of change and harm reduction) | Obtaining of treatment for alcohol and drug use and remaining in recovery Use of community resources. Ensuring that any future babies are not alcohol- and drug-affected For children, the services received include immunisations, well-child visits and therapeutic services. |
Parenting Together Project (PTP) | Couples who just became first-time parents and could use assistance in developing the father’s role in parenthood | To increase mothers' support and expectations for the fathers' involvement; to foster co-parental teamwork in the couple; and to have the couple deal more constructively with contextual factors, such as work and cultural expectations | Universal prevention | Educational intervention for first-time parents focusing on the development of fathers' knowledge, skills and commitment to the fatherhood role. The intervention consists of eight 2-hour sessions that are spread out between the second trimester of pregnancy and five months postpartum. | Positive effects on fathers' skills in interacting with their babies and their involvement on workdays. |
Parents as first Teachers /Parents as teachers (USA) | Parents of children pre-birth to 5 years old. The programme is often used as a targeted approach for families with high needs | To develop family resilience and promote positive parenting behaviours that will persist | Universal prevention (targeted at a risk group) | Parents are visited at home by a parent educator who supports them in developing their relationship with their child by highlighting the strengths in the parent–child interactions, as well as encouraging the parents to observe and be aware of the child’s development and increase the child’s school readiness. Practitioners help parents reflect on their parenting, and jointly with parents develop strategies for addressing developmental and behavioural concerns. The programme also has a community element, where parents are supported to link into community resources and regularly attend a group session. | Positive effects on parental outcome measures related to acceptance of the child’s behaviour, happiness in caring for them. Improvements in children’s adaptive behaviour, developmental status and language skills, and for the most vulnerable families in their sample, a reduction in problem behaviour. |
Preparing for life | Expectant parents living in disadvantaged neighbourhoods/ communities. All age groups of children | To create nurturing home environments by improving parental self-efficacy and well-being, ultimately promoting children's long-term school readiness and development | Targeted at a risk group | Delivered in home and community centre settings and aims to support the creation of a nurturing home environment, improve parenting outcomes in the short term (e.g., parental self-efficacy, well-being) and improve children’s school readiness in the longer term. | Enhancement of school achievement & employment. Supporting of children's mental health and well-being |
Promoting first relationships | Parents and caregivers of infants and toddlers 0–3 years of age, families at high risk of attachment disruption and with parents who themselves have experienced physical abuse | To improve the parent–infant relationship through enhanced parental sensitivity. | Targeted at risk group | Individual home-visiting programmes are covered through guided reflection on videotaped interactions between the caregiver and child, as well as through the use of parental handouts and infant cue cards. | Improves child emotional regulation and increases toddlers’ secure base behaviours through positive change in the parent–child relationship because of enhanced parental sensitivity. |
Solihull Approach Antenatal Parenting Group | Anyone expecting a baby and anyone around the mother wishing to build a strong healthy relationship with their infant. | To gain understanding of pregnancy, labour, birth and the baby in a universal group for anyone expecting a baby and for anyone around the mother wishing to build a strong healthy relationship with their infant. | Universal prevention | The programme is delivered in a group setting over a 5-week journey and can also be accessed online, covering nine modules. Ten to twelve parents are invited to attend each group. The programme provides practical information about pregnancy and birth | Increased feelings of attachment, decreased anxieties, an increased intention to breastfeed and a sense of closeness between parents and the infant . |
EIF Early Interaction Foundation Guidebook – Foundations (grade 3 or higher)
NHS Early Intervention Framework NES – Early Intervention Framework – Search (grade 3 or higher)
CEBC CEBC » Registry (1-2 (reverse scale))
Blueprints for Healthy Youth Development Blueprints Programs – Blueprints for Healthy Youth Development (model or higher)
Appendix 5. Template for the documentation of national expert discussions
Subject 1. Needs |
1. What identified risk or protective factors should be prioritized in identifying and addressing psychosocial support needs during the perinatal period now and in the future? Which currently recognized factors must be covered at minimum to ensure adequate support? What emerging needs or phenomena might arise over the next years that could significantly impact psychosocial wellbeing? Is there a specific factor or issue that stands out as critical from a national perspective in terms of impact or importance? |
Summary of national discussion: |
Subject 2. Gaps |
2. What gaps remain in our understanding of risk and protective factors in perinatal period, and which ones are nationally critical to address? Which key perinatal factors were identified in the report, and which were overlooked or underrepresented? Are there any phenomena or factors that, although not currently recognized, are likely to be significant in shaping psychosocial wellbeing (either risks or protective elements)? Are there validated interventions missing from the current mapping? |
Summary of national discussion: |
Subject 3. National issues |
Are there specific populations that require targeted support? |
Summary of national discussion: |
Appendix 6. Limitations
This report is grounded in literature and intervention searches focusing on psychosocial risk factors and psychosocial support. Due to the specificity and breadth of the topic, certain important areas, such as low birth weight or prematurity, feeding difficulties and adolescent pregnancies, have been excluded.
Despite the extensive body of research on the impact of prematurity on parent–child interaction, this topic was excluded from the present review. From an intervention standpoint, prematurity is typically addressed within specialised healthcare settings and involves complex, multidisciplinary expertise. In this review, the focus is on areas more amenable to low-threshold psychosocial support and preventive approaches.
The significant impact of feeding difficulties on parent–child interaction and the broader psychosocial well-being of the family is well recognised. However, challenges related to feeding often require the expertise of specialised healthcare professionals or multidisciplinary teams. For this reason, feeding-related issues were also excluded from the scope of the present review.
In the Nordic countries, the adolescent birth rate is low, which is why this review does not include a specific focus on adolescent motherhood. It is important to acknowledge that in some countries, including those with high-income economies, the birth rate among young mothers is significantly higher. In such contexts, various psychosocial support interventions have been developed and implemented to address the specific needs of young mothers.
While the COVID-19 pandemic had an impact on perinatal mental health, its effects are considered context-specific and time-bound. Including COVID-19-related studies could have introduced confounding factors that are not generalisable to non-pandemic conditions. The aim of this review was to identify risk and protective factors relevant to more stable and enduring healthcare and social service contexts, rather than those shaped by an exceptional global crisis. However, there is clear evidence on how the lockdowns caused by COVID-19 had a negative impact on perinatal mental health, highlighting the need for support systems in situations where normal daily life is disrupted to prevent the potential long-term effects of poor maternal mental health on infants (Wall & Dempsey, 2023).
An inclusion criterion for the search was publication in the English language. This ensured equality between the Nordic languages but may also have distorted the results in terms of the research conducted in the Nordic countries.
This review is based exclusively on meta-analyses and systematic reviews, rather than individual studies. The scope was narrowed to specific topics, excluding areas such as pandemic-related issues and feeding difficulties. A notable limitation is the lack of Nordic meta-analyses, which restricts opportunities to combine cohort data and deepen understanding of this population.
The review does not include experiential knowledge from families themselves, even though such perspectives are essential for identifying barriers to care. Furthermore, the interconnected nature of risk factors and the somewhat artificial fit into predefined domains may oversimplify complex realities. From a decision-making perspective, these limitations highlight the need for more integrated evidence, the inclusion of family experiences and region-specific analyses to inform effective policy and practice.
Most of the studies included in this review primarily focused on maternal perspectives. Although this literature review covers a wide range of risk and protective factors during the perinatal period, there are certain areas it does not address. One of the challenges in perinatal research is obtaining direct data on infants and toddlers due to their young age, which limits the scope of this review to a parent-centred perspective. While it is a valid starting point to assume that the well-being of parents is crucial for the well-being of the infant and that protective factors for parents are also relevant for the child, this review does not take into account other important aspects that are essential for infant well-being. Factors such as a generally safe and nurturing environment, consistent routines and other secure relationships are also crucial for the infant’s development and well-being, yet they fall outside the scope of this review. Early childhood education as a growth environment for young children was also excluded from the search. The search terms only partially captured the literature on interaction and early relationships. Although the search was later expanded, the authors feel that the literature reviewed does not provide a completely clear or comprehensive picture of the significance of early interaction and attachment for psychosocial well-being.
Although some research on the effectiveness of psychosocial interventions or approaches emerged in the literature, it should be noted that no separate searches were conducted specifically for psychosocial interventions; rather, these findings surfaced through the broader review process. The psychosocial intervention portal search was limited to certain information portals. There are also other organisations that collect information on interventions and assess their effectiveness, but in this review, we chose to emphasise evaluations conducted through Nordic collaboration and to use the most comparable assessment systems. The evaluation systems differ, and their effectiveness scales vary, which may introduce a risk of inconsistency in our assessment. To broaden the perspective and consider the potential implementation of international methods, well-recognised UK and US evaluation frameworks were also included. However, it is possible that some methods already implemented in the Nordic countries have not been assessed in the systems we reviewed or have not received sufficiently high effectiveness ratings. It is highly challenging to know exactly which interventions have been implemented across different regions and organisations. Our aim was to highlight those with researched evidence and that have undergone a systematic evaluation process. A key limitation of the report is that its preparation involved reviewing a vast and diverse body of material (including literature, an intervention mapping exercise, expert opinions and, as a supplement, international recommendations) within a relatively short time frame. The broad scope and limited preparation time increase the risk that the analysis and synthesis may remain somewhat incomplete, and that not all connections between phenomena or nuances offered by the data will be fully apparent.
Add Appendix 7. Abbreviations
ACE | Adverse Childhood Experiences |
ADHD | Attention Deficit Hyperactivity Disorder |
AI | Artificial Intelligence |
AND | Antenatal Depression |
ANRQ | Antenatal Risk Questionnaire |
BMI | Body Mass Index |
CBT | Cognitive Behavioural Therapy |
CEBC | California Evidence-Based Clearinghouse for Child Welfare |
COPE | Centre of Perinatal Excellence |
COVID-19 | Coronavirus Disease |
CPTSD | Complex Post-Traumatic Stress Disorder |
CS | Caesarean Section |
EBP | Evidence-Based Practice/Intervention |
EIF | Early Intervention Foundation |
EMDR | Eye Movement Desensitization and Reprocessing |
EPDS | Edinburgh Postnatal Depression Scale |
EPIS | Exploration, Preparation, Implementation, Sustainment – framework |
FASD | Fetal Alcohol Spectrum Disorders |
GAD | Generalised Anxiety Disorder |
ICD-11 | International Classification of Diseases (11th Revision) |
IPT | Interpersonal Therapy |
IPV | Intimate Partner Violence |
LGBTQ | Lesbian, Gay, Bisexual, Transgender, Queer |
LGTBQ | Variant of LGBTQ (same meaning) |
NCCMH | National Collaborating Centre for Mental Health |
NICE | National Institute for Health and Care Excellence |
NICU | Neonatal Intensive Care Unit |
OCD | Obsessive–Compulsive Disorder |
PD | Panic Disorder |
PMADs | Perinatal Mood and Anxiety Disorders |
PMH | Perinatal Mental Health |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
PSPT | Pregnancy-Specific Psychological Trauma |
PTSD | Post-Traumatic Stress Disorder |
PTSS | Post-Traumatic Stress Symptoms |
RCPsych | Royal College of Psychiatrists |
RCT | Randomized Controlled Trial |
SBU | Swedish Agency for Health Technology Assessment and Assessment of Social Services |
SMI | Serious Mental Illness |
TFPT | Trauma-Focused Psychological Therapies |
UNICEF | United Nations Children’s Fund |
WHO | World Health Organization |
Statement on the Use of Artificial Intelligence: Artificial intelligence (AI) tools were used in limited parts of this work to support the combination and organisation of certain materials. Microsoft 365 Copilot (organization‑licensed version) was used only within the organisation’s internal Teams environment for text formatting and structuring. AI-assisted methods were also applied to help with the classification of selected content and to provide preliminary language translation. The AI tool has no authorship and does not replace the author’s judgment. All final analyses, interpretations and conclusions were conducted and validated by the authors.