Photos: Jens Lindström/imagebank.sweden.se and iStock
Background and analytic approach
Background
Healthcare systems in the Nordic countries resemble each other in that they largely are owned, funded and operated by the public. The countries also resemble each other in that they have the same demographic challenges and struggle with educating and retaining health personnel. As in any country with fiscal responsibility, the Nordic countries try to contain costs as more expensive remedies for diagnosis and therapy come out of the research and innovation pipelines. At the same time, the Nordic countries nurture an ecosystem of enterprises that are active in developing medical devices, medicinal products and other health-related technologies for an increasingly globalised marketplace.
Since the advent of digital tools for storing and managing information, health authorities in the Nordic countries have embraced, and taken an active role in supporting the development and implementation of information systems to enhance their healthcare systems. Table 1 provides an overview of systems and implementation status.
Denmark | Finland | Iceland | Norway | Sweden | |
Health record systems | ✓ | ✓ | ✓ | ✓ | ✓ |
Health registries | ✓ | ✓ | ✓ | ✓ | ✓ |
National patient portals | ✓ | ✓ | ✓ | ✓ | ✓ |
Laboratory information systems | ✓ | ✓ | ✓ | ✓ | ✓ |
Imaging information systems | ✓ | ✓ | ✓ | ✓ | ✓ |
Table 1. Status of information system implementations in the Nordic countries.
The Nordic Committee of Senior Officials for Health and Social Affairs (ÄK-S) of the Nordic Council of Ministers (NCM) established the eHealth group (the Nordic Council of Ministers’ eHealth group) in 2011 to ensure knowledge transfer between the Nordic countries, and help to strengthen the global leadership position of the region in the eHealth area.
The NCM e-health group supports a Nordic e-Health Standardization group and the Nordic e-health Research Network (NeRN)
The primary objective for the current mandate period is to develop and pilot an updated set of indicators that can be used to assess and compare the impact of national-level digital health programmes in the Nordic countries.
Analytic approach
The previous policy analysis and indicator development activities
Hyppönen H, Faxvaag A, Gilstad H, Hardardottir G, Jerlvall L, Kangas M, et al. Nordic eHealth Indicators. TemaNord 2013 522. 2013.
Hyppönen H, Faxvaag A, Gilstad H, Hardardottir GA, Jerlvall L, Kangas M, et al. Nordic eHealth Indicators: Organisation of Research, First Results and Plan for the Future. Stud Health Technol Inform. 2013;192:273–7.
Hyppönen H, Kangas M, Reponen J, Nøhr C, Villumsen S, Koch S, et al. Nordic eHealth benchmarking. Nordic Council of Ministers; 2015.
Hyppönen H, Koch S, Faxvaag A, Gilstad H, Nohr C, Hardardottir GA, et al. Nordic eHealth benchmarking : From piloting towards established practice (2017) [Internet]. Nordisk Ministerråd; 2017 [cited 2023 Aug 17]. Available from: https://urn.kb.se/resolve?urn=urn:nbn:se:norden:org:diva-4840
Price M, Lau F. The clinical adoption meta-model: a temporal meta-model describing the clinical adoption of health information systems. BMC Med Inform Decis Mak. 2014 May 29;14(1):43.
There are however many other professional roles and groups that are to benefit from Health information systems and the healthcare data that accumulates in them. In our 2012 and 2016 reports we introduced the terms ‘stakeholder’ and ‘stakeholder engagement’, and assessed each country's eHealth policy according to which stakeholders were mentioned and how they were to benefit from the activities and objectives described.
In our 2020 report
Nöhr C, Faxvaag A, Tsai CH, Hardardottir GA, Hyppönen H, Andreassen HK, et al. Nordic eHealth Benchmarking Towards evidence informed policies (2020) [Internet]. 2020 [cited 2023 Aug 17]. Available from: https://www.norden.org/en/publication/nordic-ehealth-benchmarking-0
Table 2. Personas identified (extract from the 2020 report)
Personas | Goals (examples) | Fears / challenges (examples) |
Citizen | Access to own data and to the data of next-of-kin. Access to treatment and appointments. | Fears missing valuable information concerning the treatment of family members. She does not fear loss of privacy but is more afraid of losing overview of her data. |
Patient | To feel safe. To experience as few healthcare handovers as possible. | Easily confused, the patient has a low confidence in data safety and IT in general. Fears losing ability to live independently and taking care of herself. |
Clinician | Reliable health information systems – high stability, security and confidentiality. To deliver the best possible quality of services – medical measures, access to clinical guidelines. | That patient data in different health sectors are not being shared and used to provide the best possible treatment for patients. To be unjustifiably accused of malpractice by patients squeezed by the healthcare system. To mishandle his management responsibilities due to lack of insight. |
Policy Maker | Wants clear messages and need focused information. Need for knowledge about things that work. Requires knowledge-based facts – e.g. knowledge about international trends. | Lack of overview into how the policy goal implementations are progressing, what are the differences between regions. Afraid of being misunderstood and making decisions based on misinformation. |
Industry CEO | Develop a deep understanding of health systems. To create a competitive, market-leading, product. To obtain some of the value that lies in the data that are stored in the system. | Losing market shares. Bad publicity for products deployed at customer sites. |
Politician | Wish to initiate changes in the use of ICT in a good way. Wants that every deviation and breach in security must be documented. Wants an overview of safety cultures, resources spent on safety and security | Holistic use of ICT solutions – system integration. The effects of using eHealth – dissemination. Reducing travel and transport expenditures for patients and health providers. Reducing the length of stay in hospitals. Improve empowerment of patients. |
Health institution manager | Analytics of indicators – used as decision support. Staff perception of useful systems. Balance staff and customer satisfaction. | Regulatory concerns (IT-security). Report upwards (regional administration and politicians). Budget cuts and whimsical politics. High cost of IT employees. |
Researcher | To publish scientific papers and reports on his research work. To keep up to date with recent developments within his field. | Violating the confidentiality of the research data he has access to. Basing his work on obsolete data. |
IT-professional | To manage his projects successfully, including sharing information regarding the capability and strengths of the delivered solution. To understand the expectations and needs of the project stakeholders. | Failure to reach project deadline. Failure to meet stakeholder expectations. Delivery of a system that does not comply with requirements, including those of legislative and cyber/information security character. He is challenged in understanding the clinical work context of the users. |
Since our 2020 report, it has become increasingly clear that the value of an information system extends beyond its value for the users of the system. The information that accumulates through use of the system has a value in itself, a value that should be preserved when one EHR system is replaced by a newer system. State of the art in healthcare information system engineering is now to enhance the value of the information that accumulates by structuring the information and in using terminology systems such as ICD-10 and Snomed-CT. Another major trend is that EHRs not only are used to document care and store care recordings but increasingly used to distribute relevant knowledge to the clinician user at point of care. This means that EHR-systems contain representations of the knowledge that is to be applied, representations that need to be governed and maintained. A third development is the introduction of new means of analysing data (e.g. machine learning) and new entities that are to learn from the data (i.e. machines). Taken together, these advancements in health information system engineering point towards a future where these systems become more and more integral to the healthcare system they are to serve. These developments will further add to the value. In the near future we will see health information systems that are capable of transforming how health problems are approached, surveilled, analysed, solved and followed-up as virtualized care is becoming a realistic alternative to consulting the patient in a consultation room.
In the current round of policy analysis and indicator development we shall also use a system theoretic approach. We shall use system theory to describe healthcare systems and health ecosystems and to define areas where new indicators might be needed. We shall stick to the principle that an information system tool shall be evaluated as to how it contributes to value-creation. We shall think of the system as a tool that has value for practitioners at all levels in a healthcare system. That includes the new and emerging roles that relate to knowledge management (e.g. configuration of workflows, clinical decision-support, digitised care pathways, population health and health operations management). The same relates to entities, practices and routines that relate to working with healthcare data to assess the value of the care that was provided, to validate the knowledge that was used in knowledge-based care and to enable contributors to learn by assessing the actual outcome of their work.
System theory and its relevance to healthcare systems
According to the Merriam-Webster dictionary, a system can be described as “a group of interacting or interrelated elements that act according to a set of rules to form a unified whole”. A system, surrounded and influenced by its environment, is described by its boundaries, structure and purpose and expressed in its functioning. Systems are the subjects of study of systems theory and other systems sciences
Adam T. Advancing the application of systems thinking in health. Health Res Policy Syst. 2014 Aug 26;12(1):50.
Healthcare systems, health ecosystems and their value chains
The goal of any healthcare system is to protect its users when their health is impacted by damage, disease or aging. They achieve this by applying knowledge, medicines, medical devices and health personnel’s skills. As in any system with a finite amount of resources, healthcare systems must optimize its activities so they get the most value out of the resources. Healthcare systems have ethics. They are goal-directed and therefore have value chains. Healthcare systems interact with institutional entities in a surrounding health ecosystem. Irrespective of practice and location in the system, you cannot aspire to contribute anything of value unless you have a knowledge-based approach, state your intended outcomes and organise the work so that you get to learn from the outcomes that actually were achieved.
The model outlined here is illustrated with examples from the healthcare sector but also holds for the social care setting. The main difference is the risk exposure (explained below) both on the patient/client side and on the side of the health or care professional.
The healthcare value chain
If we define a health problem as a problem that affects, or might affect someone’s health, most jurisdictions define a patient as a person that asks a health professional for help with a health problem. In this context, healthcare is an activity that is restricted to health professionals. A health professional is then a person that is authorised or licensed to provide healthcare. Possessing a health problem is associated with risk. Asking a health professional for help with the problem is then a means of dealing with the risk by sharing it with another person (the health professional). Carrying out healthcare then implies that the patient assigns a care mandate to the health professional that the health professional subsequently accepts. Healthcare is then a mandated activity that is carried by a health professional to analyse, explain, mitigate and possibly eliminate the health problem. A care mandate can be implicit. Healthcare also includes activities that the patient carries out in an agreement with a health professional such as turning up for a consultation, taking a prescription, reporting on side effects or reporting an outcome. The term self-care should denote other health-related activities that are initiated and fully controlled by the citizen or next-of-kin.
In the context of (professional) care, problem solving can be described as an iterative, decision-centred process that starts with collecting (patient-specific) data about the problem.
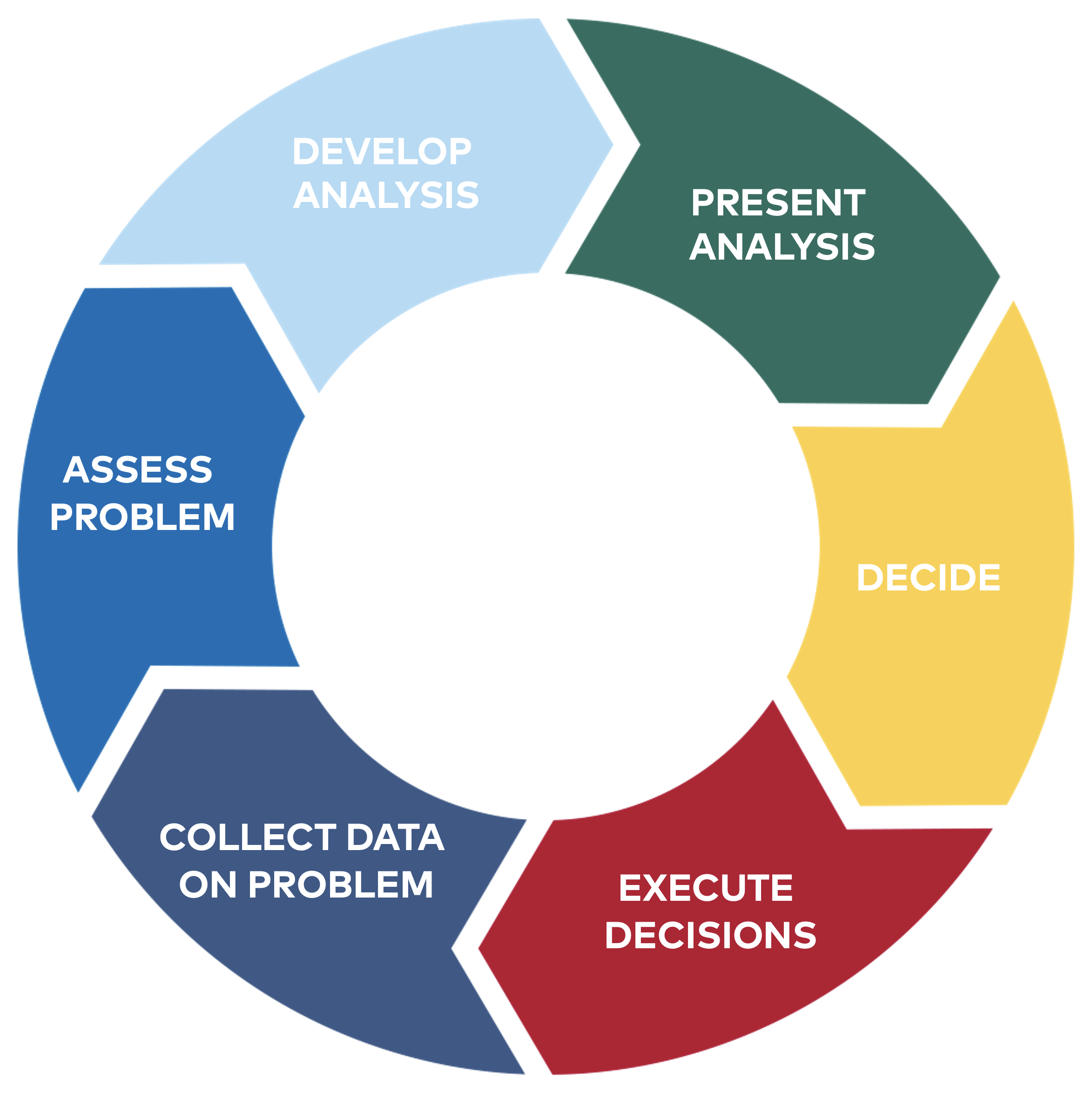
Figure 1. The problem-solving cycle.
Problem-specific data illuminates the problem and are subsequently used to search for, choose and present the best explanation. Assessing the problem, developing and subsequently presenting an analysis is described as medical problem-solving or in the scientific literature
Elstein AS, Schwarz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ. 2002 Mar 23;324(7339):729–32.
Weed LL. Medical records that guide and teach. N Engl J Med. 1968 Mar 14;278(11):593–600.
Deciding on the knowledge that is to be applied to eliminate or mitigate the problem is described as clinical decision-making
Elstein AS, Schwarz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ. 2002 Mar 23;324(7339):729–32.
Gulbrandsen P, Clayman ML, Beach MC, Han PK, Boss EF, Ofstad EH, et al. Shared decision-making as an existential journey: Aiming for restored autonomous capacity. Patient Educ Couns. 2016 Sep 1;99(9):1505–10.
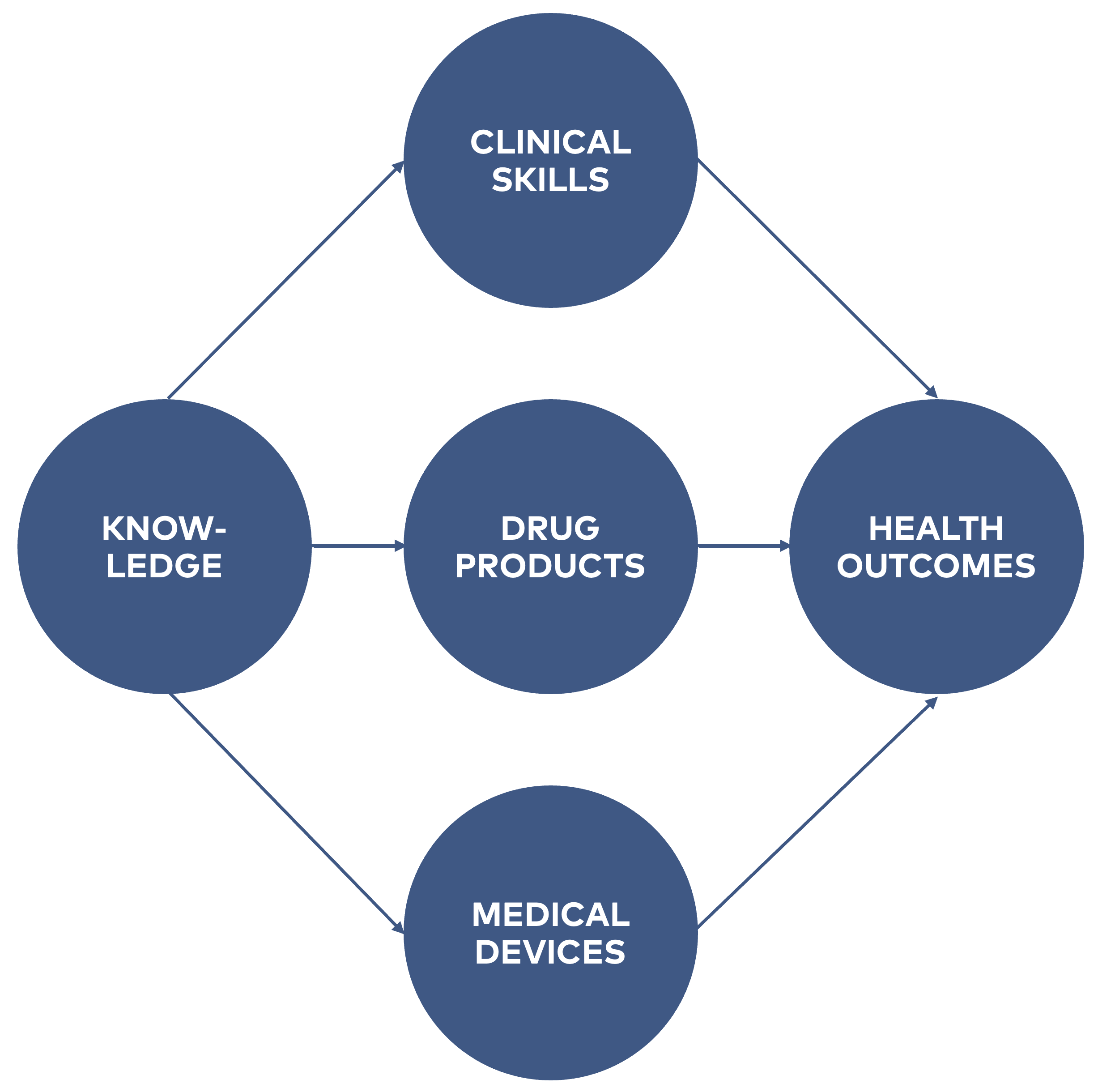
Figure 2. Application of knowledge to achieve valuable health outcomes.
For some health problems, the problem is access to health professionals that are trained in recognising that particular problem and possess the clinical skills that are required to provide knowledge-based care to the patients (e.g. access to speciality care). For other health problems, the problem is that there are no truly valuable knowledges to apply. In the case of grave and immediate risk, the best chance for the patient can be to test out of experimental therapy in an ongoing clinical trial. Here, access to a knowledge development infrastructure and services is paramount. A third group of patients are those that have or are about to develop a rare disease. Since the patients are so few, clinicians never get enough training in recognising them. Likewise, it is notoriously hard to team up with other clinicians to develop new knowledge about the disease by establishing and populating a sufficiently large disease-specific registry.
Table 3. Overview of value chains in healthcare systems and health ecosystems
Value chain | Input | Outcome | Reaps the value | Main constraint |
Healthcare | Health problem | Years to life Life to years | Citizen | Availability of expertise |
Research and engineering | Data about the health problem | Applicable knowledge, medicines and medical devices | Knowledge user Vendor of product | Availability of data from the domain |
Education and training | Situations where the health problems are dealt with by health professionals | Competence | Health Institutions | Availability of situations |
The research value chain
Biomedical research and development (R&D) can be described as the use of the scientific method to develop knowledge that can be applied to understand, explain or mitigate a health problem. Carrying out a biomedical R&D project always requires access to data from patients that possess the health problem and / or biological specimens sampled from the same patients. When the scientific investigation is a randomized clinical trial, those who carry out the experiment also need to interact with the patient. Carrying out a scientific investigation from defining the research problem to publishing a valid scientific result is usually an undertaking of a university or another research institution. The Covid pandemic clearly demonstrated that international collaborations are required to build sufficiently large cohorts, plan and realize the R&D that will bring about the vaccine products and other knowledges that were needed.
In general, knowledge that comes out of a biomedical R&D project can a) be applied to better understand the nature of disease; b) incorporated in guidelines, expressed in decision rules or clinical workflows; c) incorporated in methods or devices that can be used to portray the nature of a disease in greater detail (e.g. a diagnostic or prognostic test); d) applied to develop a candidate new drug product or medical device or e) applied as documentation that a drug product or medical device is of sufficiently large value to be taken into regular clinical use. Since working with health problems is dealing with risk, and mitigating risk by exposing the patient to drug or medical device products adds new risks, the true (realised) value of the product cannot be assessed without obtaining outcome data.
The knowledge development value chain is constrained by several factors. Many of them have to do with limited access to data about individual patients’ health problems and how these are dealt with by health professionals.
The education and training value chain
A health professional is a person that is authorised or licensed to provide healthcare. Elstein
Epstein RM, Hundert EM. Defining and Assessing Professional Competence. JAMA. 2002 Jan 9;287(2):226–35.
Most jurisdictions recognize around 30 different kinds of health personnel and educational programs. Basic health professional education takes place at universities. The educational programs provide a theoretical basis on top of which the students start developing their own experience-based insights. Exposure to real patients and their health problems occurs through bedside training in health institutions. Health institutions therefore also count as educational institutions. There are around 50 different medical specialities. A medical doctor that undergoes speciality training has acquired the right to develop a deeper insight in a particular subset of the biomedical knowledge base (e.g. Infectious diseases), develop the clinical skills that are specific for the specialty and develop experience-based knowledge on the same patient groups. Most of the learning occurs through supervised exposure to a sufficiently large number of patients with a relevant health problem.
From a systems and HR perspective, there are many problems with developing and maintaining a competent workforce. Once health professionals have become fully capable at what they are doing, keeping them competent requires a commitment to lifelong learning, both from the employer and the employee side. The professionals' need for training is real, because careers in healthcare can be long. At the moment, after the middle-aged healthcare professionals’ graduation several new treatments have been introduced to achieve health benefits, for example, biological drugs have created new treatment options for rheumatoid arthritis patients, and many surgical treatments have been omitted from the treatment as the treatment of the disease can be influenced already at an early stage. Changes in evidence-based care also affect healthcare professionals other than physicians, therefore evolving training throughout the different professional groups is essential. Changes in care practices have an impact on workflow and, ideally, EHRs are modified to support the healthcare professionals' workflows.
A health system is also a system for matching health problems to professionals with the right expertise. For some health problems, there aren’t enough cases for professionals to develop the experience-based knowledge that is needed. Also, the need for (continuous) education and training is heavily influenced by what happens in the knowledge development value chain. Research and development may bring about a new kind of medical device (e.g. stents for blocking out stenoses in coronary arteries), but this therapy cannot be applied on the relevant patients unless professionals undergo the required training.
EHRs and other digital health systems undoubtedly influence learning. Health professionals both develop and practice their problem-solving and decision-making skills by means of the EHR. As they learn while they practice, they embed their skills with the EHR tool at hand. The EHR is also key to learning from data on the true outcomes of your work (e.g. patient-reported outcomes). Finally, decision-support and knowledge-support tools in the EHR are also sources of learning.
Figure 3. Illustration of a Health ecosystem. Adapted from Hasselgren
Hasselgren A, Kralevska K, Gligoroski D, Pedersen SA, Faxvaag A. Blockchain in healthcare and health sciences—A scoping review. Int J Med Inf. 2020;134:104040.

A healthcare system will always be constrained by the resources that are available. There will never be enough funding. There will always be knowledge that a healthcare system cannot afford to apply. There will always be healthcare situations devoid of knowledges to apply. There will always be limitations to professional training and availability of expertise. As a system of entities that are networked to each other, there will be additional problems at the outermost parts of the network (e.g. attracting and retaining personnel at the most remote healthcare organisations).
Correspondingly, there are high-level healthcare system problems and challenges where information system infrastructures and tools are the only solution. Given the rapid advancements in the field, we must now expect a rollout of ever-more capable health information systems. This development has implications for digital health policy making as well as for how we are to evaluate this next generation of systems and infrastructures.
References
Adam T. Advancing the application of systems thinking in health. Health Res Policy Syst. 2014 Aug 26;12(1):50.
Elstein AS, Schwarz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ. 2002 Mar 23;324(7339):729–32.
Epstein RM, Hundert EM. Defining and Assessing Professional Competence. JAMA. 2002 Jan 9;287(2):226–35.
Gulbrandsen P, Clayman ML, Beach MC, Han PK, Boss EF, Ofstad EH, et al. Shared decision-making as an existential journey: Aiming for restored autonomous capacity. Patient Educ Couns. 2016 Sep 1;99(9):1505–10.
Hasselgren A, Kralevska K, Gligoroski D, Pedersen SA, Faxvaag A. Blockchain in healthcare and health sciences—A scoping review. Int J Med Inf. 2020;134:10404.
Hyppönen H, Faxvaag A, Gilstad H, Hardardottir G, Jerlvall L, Kangas M, et al. Nordic eHealth Indicators. TemaNord 2013 522. 2013.
Hyppönen H, Faxvaag A, Gilstad H, Hardardottir GA, Jerlvall L, Kangas M, et al. Nordic eHealth Indicators: Organisation of Research, First Results and Plan for the Future. Stud Health Technol Inform. 2013;192:273–7.
Hyppönen H, Kangas M, Reponen J, Nøhr C, Villumsen S, Koch S, et al. Nordic eHealth benchmarking. Nordic Council of Ministers; 2015.
Hyppönen H, Koch S, Faxvaag A, Gilstad H, Nohr C, Hardardottir GA, et al. Nordic eHealth benchmarking : From piloting towards established practice (2017) [Internet]. Nordisk Ministerråd; 2017 [cited 2023 Aug 17]. Available from: https://urn.kb.se/resolve?urn=urn:nbn:se:norden:org:diva-4840
Nöhr C, Faxvaag A, Tsai CH, Hardardottir GA, Hyppönen H, Andreassen HK, et al. Nordic eHealth Benchmarking Towards evidence informed policies (2020) [Internet]. 2020 [cited 2023 Aug 17]. Available from: https://www.norden.org/en/publication/nordic-ehealth-benchmarking-0
Price M, Lau F. The clinical adoption meta-model: a temporal meta-model describing the clinical adoption of health information systems. BMC Med Inform Decis Mak. 2014 May 29;14(1):43.
Weed LL. Medical records that guide and teach. N Engl J Med. 1968 Mar 14;278(11):593–600.